J Res Clin Med. 13:35304.
doi: 10.34172/jrcm.025.35304
Original Article
Psychometric evaluation of the questionnaire assessing primary health care providers’ knowledge and attitudes toward gender dysphoria
Ali Reza Shafiee-Kandjani Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing, 1 
Yaghoub Khodabandeh Data curation, Investigation, Validation, Writing – original draft, Writing – review & editing, 1
Behzad Shalchi Conceptualization, Formal analysis, Methodology, Software, Supervision, Writing – review & editing, 1, *
Habibeh Barzegar Data curation, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing, 1
Author information:
1Research Center of Psychiatry and Behavioral Sciences, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
Gender dysphoria is one of the significant challenges in healthcare systems, and primary healthcare providers play a key role in caring for and referring these individuals. However, their insufficient knowledge and attitudes may lead to inadequate care. Given the lack of a standard Persian tool for measuring these variables, this study aimed to psychometrically evaluate a questionnaire assessing the knowledge and attitudes of primary healthcare providers regarding gender dysphoria.
Methods:
This descriptive cross-sectional study was conducted in 2024 in Tabriz, involving three phases: translation, back-translation, validity, and reliability. The study sample for content validity included 15 experts, 30 healthcare providers for reliability, and 205 primary healthcare providers for construct validity. The research tool consisted of questionnaires assessing attitudes and knowledge about transgender individuals, which were translated into Persian and culturally adapted. Content validity was evaluated using content validity ratio (CVR) and content validity index (CVI), and construct validity was assessed through confirmatory factor analysis (CFA). The reliability was calculated using Cronbach’s alpha coefficient and the intra-class correlation coefficient (ICC).
Results:
The results of this study indicated that the overall CVI was 0.81 and the CVR was 0.93. For the knowledge section, CVI was 0.76 and CVR was 0.94, while for the attitude section, CVI was 0.85 and CVR was 0.91. In confirmatory factor analysis, the factor loadings for the attitude section were above 0.30, but some questions in the knowledge section had factor loadings lower than 0.30. The comparative fit index (CFI), goodness of fit index (GFI), normed fit index (NFI), and root mean square error of approximation (RMSEA) were 0.96, 0.90, 0.85, and 0.057, respectively, all indicating a good model fit. Additionally, the Cronbach’s alpha coefficient for the entire questionnaire was 0.86, and for the knowledge and attitude sections, it was 0.65 and 0.88, respectively. The ICC obtained from the test-retest method was 0.76, confirming the reliability of the questionnaire.
Conclusion:
The results of this study showed that the tool for measuring the knowledge and attitude of primary healthcare providers regarding gender dysphoria has good validity and reliability. The confirmatory factor analysis results indicated that the two-factor structure (knowledge and attitude) fits well, although some items in the knowledge section had lower factor loadings. This questionnaire can be helpful in designing educational and research programs in this area.
Practical Implications:
The questionnaire could be used as a screening tool in educational programs related to gender dysphoria, assessing the impact of educational interventions, and evaluating educational needs in healthcare policy-making.
Keywords: Gender dysphoria, Healthcare providers, Knowledge, Attitudes, Validity, Reliability
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This study was supported by Research Center of Psychiatry and Behavioral Sciences at Tabriz University of Medical Sciences.
Introduction
Gender dysphoria, as defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), refers to a marked incongruence between an individual’s experienced or expressed gender and the gender assigned at birth.1 Accurate data on gender dysphoria are unavailable. However, it appears to be more common among men, with estimates suggesting one in 10,000 men and one in 30,000 women may be affected.2 Overall, the number of individuals with gender dysphoria is estimated to range from one in 30,000 to one in 100,000 individuals, varying across different societies.3 In Iran, approximately 2,500 registered individuals have been officially diagnosed with gender dysphoria, based on available data from relevant institutions. 2 Gender dysphoria does not have a single known cause. It arises from the interaction of biological, familial, psychological, and social factors.4,5 Biological and psychological factors such as prenatal stress, genetic and hormonal conditions, neurological issues, and central nervous system disturbances are among the most significant contributors to this condition.6 Additionally, social factors such as an overly close relationship with the mother and distance from the father in boys, or a depressed mother during the early months of life and absent, unsupportive fathers in girls, may increase the likelihood of gender dysphoria.7 According to DSM diagnostic criteria, the core features of gender dysphoria include a strong, persistent desire to identify with the opposite gender (not motivated by cultural or social advantages), clear evidence of ongoing distress related to the current gender role, and a sense that the assigned gender role does not align with one’s feelings, resulting in significant distress or impairment in social, occupational, or other areas of functioning.8 Individuals experiencing this distress often struggle to align their gender expression with traditional binary social roles (man or woman), which can lead to strained relationships with family, peers, and friends, social rejection, interpersonal conflicts, depression, anxiety, substance abuse, reduced well-being, low self-esteem, and an increased risk of self-harm or suicide.9 Individuals with gender dysphoria typically seek care from primary healthcare providers, endocrinologists, or mental health professionals.10 In some cases, gender dysphoria may be the primary reason for seeking care, while in others, it may co-occur with other mental health issues. Appropriate referral and attention to the individual’s condition are essential to establish a robust support system.11 Such referrals require primary healthcare providers to possess adequate knowledge and attitudes toward gender dysphoria. According to the Knowledge-Attitude-Behavior model, greater knowledge leads to attitude changes, ultimately resulting in effective behavioral shifts.12,13 However, in many parts of the world, gender-affirming healthcare is either unavailable or difficult to access. Even when accessible, individuals with gender dysphoria often encounter healthcare providers who, due to inadequate training and negative biases, deliver substandard care.14,15 A 2017 qualitative study on healthcare for transgender people reported that 45.7% of individuals observed inappropriate behavior or mockery from medical staff, 8.6% were excluded from treatment by a healthcare provider, and 62.9% experienced staff refusing to use their correct pronouns.16 Thus, knowledge and behavioral sensitivity among healthcare providers regarding gender dysphoria remain significantly lacking.17 To enhance the knowledge, attitudes, and behaviors of healthcare providers in this area, it is first necessary to assess their current levels using valid tools, followed by tailored educational interventions. In recent years, tools such as the 15-item Medical Practitioner Attitudes Toward Transgender Patients Scale (MP-ATTS)18 for assessing attitudes and the 13-item Medical Practitioner Beliefs and Knowledge about Treating Transgender Patients (MP-BKTTP)19 for evaluating medical beliefs and general knowledge have been used in various countries. Both questionnaires employ a 5-point Likert scale and demonstrate acceptable internal reliability. However, no standardized Persian tool exists in Iran to assess healthcare providers’ attitudes toward gender dysphoria. Given that primary healthcare providers in Iran are often the first point of contact for caring for gender dysphoria, and considering the absence of a validated Persian instrument, this study aimed to psychometrically evaluate a questionnaire assessing the knowledge and attitudes of primary healthcare providers regarding gender dysphoria. The integration of the two original instruments—MP-ATTS and MP-BKTTP—was guided by both theoretical and practical considerations. Theoretically, based on the Knowledge-Attitude-Behavior model, knowledge and attitudes are interconnected and jointly influence the care behavior of providers. Practically, combining both tools into a single, culturally adapted instrument enabled a more comprehensive and efficient assessment of these two critical domains in the Iranian context.
Methods
This descriptive cross-sectional study was conducted in 2024 at Tabriz University of Medical Sciences in three stages: translation and back-translation, validity assessment, and reliability evaluation. The study population for content validity included 15 experts (psychiatrists, psychologists, and health education specialists). For construct validity, assessed via confirmatory factor analysis (CFA), data from 205 primary healthcare providers in Tabriz were analyzed. Internal consistency was evaluated with 205 participants, and test-retest reliability was assessed with 30 primary healthcare providers. Participants were selected based on inclusion criteria, which included employment as a community health worker, health caregiver, psychologist, family physician, or nutritionist in selected Tabriz health centers and willingness to participate. Individuals unwilling to continue participation were excluded.
Research tool
The research tool was a scale for assessing healthcare disparities among transgender individuals, adapted and validated for Iranian culture. The combination of the two questionnaires into a single instrument was based on the conceptual alignment of knowledge and attitude constructs in gender dysphoria care and the need for an integrated tool tailored for primary healthcare settings in Iran.
It combined two questionnaires: 1. MP-ATTS: A 15-item survey to measure attitudes toward transgender individuals, with 6 reverse-coded items (higher scores indicate more positive attitudes). Its reliability was acceptable (0.92).18 2. MP-BKTTP: A 13-item survey assessing medical beliefs and general knowledge about treating transgender patients, with 6 reverse-coded items (higher scores indicate more positive beliefs and knowledge). Its internal reliability was 0.94.19
Translation, back-translation, and cultural adaptation
The research team translated the questionnaires into Persian and reviewed the content for cultural adaptation. The cultural adaptation process involved modifying some items—especially those relating to sensitive attitudes toward transgender individuals—to use culturally appropriate language without altering their conceptual meaning. Definitions of key terms such as “gender dysphoria (transgender)” and “cisgender” were incorporated to enhance respondent understanding. After revisions by an English language expert, the Persian version was finalized and back-translated into English by another specialist. Following necessary adjustments, the final version was reviewed and approved by the research team for validity and reliability testing.
Content validity assessment
Content validity was evaluated using opinions from 15 experts in psychiatry, psychology, and health education, selected via purposive non-random sampling. Both qualitative and quantitative methods were employed. Qualitatively, experts reviewed the items for grammar, appropriate wording, and proper placement, providing feedback for revisions. Quantitatively, content validity was assessed using content validity ratio (CVR) and content validity index (CVI). For CVR, experts rated each item on a three-point scale (essential, helpful but not essential, not necessary), with results calculated per Lawshe’s table (CVR ≥ 0.49 deemed acceptable for 15 experts). For CVI, items were rated for relevance on a four-point scale (1 = not relevant to 4 = highly relevant), with scores aggregated as the proportion of ratings of 3 or 4, requiring a CVI ≥ 0.79 for acceptance.
Construct validity assessment
Construct validity was examined using CFA with LISREL 8.5 software. Factor loadings were analyzed in standardized estimates, with values closer to 1 indicating stronger relationships between observed variables (items) and latent constructs. Loadings below 0.3 were considered weak and excluded, while 0.3–0.6 were acceptable, and above 0.6 were highly desirable. Significance was tested using t-values, with t > 1.96 indicating a significant relationship. Model fit was assessed using indices such as chi-square, root mean square error of approximation (RMSEA), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), comparative fit index (CFI), normed fit index (NFI), and non-normed fit index (NNFI).
Although the chi-square test was significant (χ2 = 474.54, P < 0.001), which may indicate a less-than-perfect fit, especially in large samples, this index is known to be sensitive to sample size. Therefore, the overall model fit was primarily evaluated based on other fit indices, including CFI, GFI, RMSEA, AGFI, NFI, and NNFI, all of which met the commonly accepted thresholds for an adequate model fit. This approach aligns with standard practices in CFA.
Reliability assessment
Internal consistency was evaluated using Cronbach’s alpha, based on responses from 205 primary healthcare providers. Test-retest reliability was assessed by having 30 providers complete the questionnaire twice, one month apart, with ICC calculated using SPSS version 26.
Results
The study results are organized into sections: translation and back-translation, content validity, construct validity, and reliability.
Translation and back-translation
After initial translation and cultural adaptation, revisions were applied, and the Persian version was back-translated into English. Following the final review and approval by the research team, the initial questionnaire with 28 items (13 for knowledge, and 15 for attitudes) was prepared.
Content validity
Quantitative content validity yielded an overall CVI of 0.81 and CVR of 0.93, indicating satisfactory validity. For the knowledge section, the CVI was 0.76 and the CVR was 0.94; for the attitude section, the CVI was 0.85 and the CVR was 0.91. Qualitative feedback from experts led to minor revisions, and ultimately, content validity was confirmed.
Construct validity
Participants included 205 primary healthcare providers from Tabriz, with a mean age of 40.13 (SD = 6.83) years. Most were female (96.6%), married (83.4%), held bachelor’s degrees (71.1%), and worked as health caregivers (73.2%). Demographic details are in Table 1.
Table 1.
Demographic characteristics of study participants (N = 205)
|
Qualitative variables
|
|
Frequency
|
Percent
|
| Gender |
Male |
7 |
3.4% |
| Female |
198 |
96.6% |
| Marital Status |
Single |
34 |
16.6% |
| Married |
171 |
83.4% |
| Education |
Associate degree |
11 |
5.4% |
| Bachelor’s |
145 |
71.1% |
| Master’s |
28 |
13.7% |
| PhD |
20 |
9.8% |
| Occupation |
Health caregiver |
150 |
73.2% |
| Psychologist |
11 |
5.4% |
| Physician |
10 |
4.9% |
| Nutritionist |
34 |
16.6% |
|
Quantitative variables
|
|
Mean
|
SD
|
| Age |
|
40.13 |
6.83 |
| Work experience |
|
13.04 |
6.14 |
CFA results indicated all attitude items had factor loadings > 0.3, indicating an acceptable correlation with the latent construct. Several knowledge items had loadings < 0.3, suggesting a weaker correlation (one, two, four, five, six, seven, eight, nine). Details are shown in Figure 1.
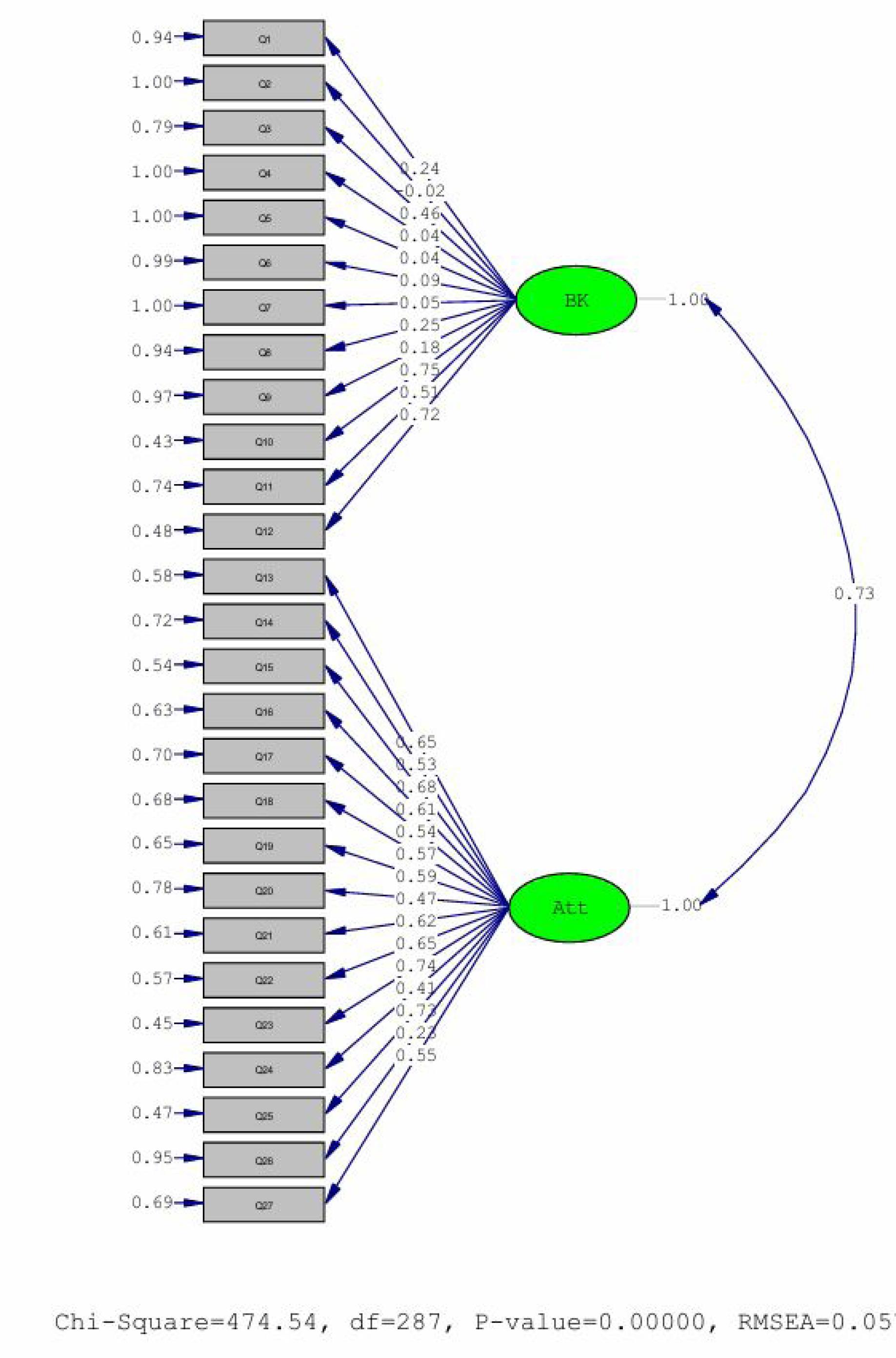
Figure 1.
Confirmatory factor analysis model in standardized estimates
.
Confirmatory factor analysis model in standardized estimates
Confirmatory factor analysis model in significance
The examination of the significance of the factor loadings, based on the software output, indicates that all factor loadings for the manifest variables related to the attitude factor are significant at the 0.05 level (with t-values greater than 1.96). However, the factor loadings for some manifest variables (questions two, four, five, six, seven) related to the knowledge factor were not significant (with t-values less than 1.96), and these are marked in red.
Based on the values obtained for the goodness-of-fit indices, the model fit was also found to be satisfactory. The chi-square index was significant (χ2 = 474.54, P value< 0.001). Additionally, the chi-square to degrees of freedom ratio was 1.65, which is less than the critical value of 3. The CFI was calculated to be 0.96, which is above the threshold of 0.90 and close to 0.95, indicating a good model fit. Furthermore, the values of the GFI and the NFI were 0.90 and 0.85, respectively. Moreover, the RMSEA index was found to be 0.057, which is one of the critical model fit indices and indicates a satisfactory model fit. More information regarding the goodness-of-fit index is provided in Table 2.
Table 2.
Goodness-of-fit indices
|
Chi-square value
|
df
|
RMSEA
|
CFI
|
GFI
|
AGFI
|
NFI
|
NNFI
|
| 474.54 |
287 |
0.057 |
0.96 |
0.85 |
0.81 |
0.90 |
0.95 |
df: degree of freedom, RMSEA: Root mean square error of approximation, CFI: Comparative fit index, GFI: Goodness of fit index, AGFI: Adjusted goodness of fit index, NFI: Normed fit index, NNFI: Non-normed fit index
Reliability
Cronbach’s alpha for the entire questionnaire was 0.86, with 0.65 for knowledge and 0.88 for attitudes, confirming internal consistency. The ICC from the test-retest was 0.76, verifying reliability.
Discussion
The present study aimed to examine the psychometric properties of a questionnaire designed to assess the knowledge and attitudes of primary healthcare providers regarding gender dysphoria. The results of the analyses indicated that the questionnaire possesses satisfactory validity and reliability, making it a valid tool for measuring knowledge and attitudes in this domain. In this study, the content validity of the questionnaire was confirmed based on the CVR and CVI, meaning that all items were deemed valid by experts. This finding demonstrates the appropriateness of the questionnaire items in relation to the concepts being measured. However, the qualitative review process led to minor revisions in some items, highlighting the importance of considering cultural differences in the design of the assessment tool.20 The results of the CFA indicated that the two-factor structure of the tool (comprising knowledge and attitude dimensions) generally had a good fit. However, some items in the knowledge section, particularly items 2, 4, 5, 6, and 7, had factor loadings below 0.3, which may indicate conceptual complexity within this dimension. It is important to note that several of these items also exhibited non-significant t-values in the CFA, suggesting that they either do not fully align with the core knowledge construct or were not adequately understood by the participants. Nevertheless, these items were retained in the final version of the questionnaire due to their conceptual importance in covering key aspects and essential subdomains of knowledge about gender dysphoria that are not reflected by other items. This decision was made based on expert consensus during the content validation phase, as removing these items could have reduced the scope and depth of the knowledge construct. Considering the importance of improving model fit and measurement precision, it is recommended that future studies with larger and more diverse samples further investigate the performance of these items, and revise, replace, or remove them as needed to enhance the instrument’s validity. In similar studies, low correlations of some knowledge items with the overall construct are often attributed to factors such as respondents’ prior familiarity with the topic or the lack of specific educational frameworks.21 On the other hand, all items related to attitude had factor loadings above 0.3, indicating a strong correlation with the latent variable and suggesting that the attitude factor has a stable structure among primary healthcare providers. This finding aligns with previous research, where attitudes typically exhibit greater consistency compared to knowledge.22 The Cronbach’s alpha coefficient for the entire questionnaire (0.86) indicated good internal consistency. However, the coefficients for the subscales showed differences, with the reliability coefficient for the attitude section (0.88) being higher than that for the knowledge section (0.65). This difference may stem from the greater stability of attitudes compared to knowledge, as well as the variability in knowledge levels among primary healthcare providers, which can lead to increased response dispersion and a lower Cronbach’s alpha.23,24 Overall, in line with previous research and considering the limited knowledge of primary healthcare providers regarding gender dysphoria, there is a need for targeted education in this area.25,26 Additionally, incorporating formal education into the training programs of primary healthcare providers is essential.27 The questionnaire developed in this study can be used to assess the knowledge and attitudes of primary healthcare providers regarding gender dysphoria, particularly in educational programs and related research. This questionnaire can serve as a tool to evaluate the effectiveness of educational interventions designed to improve the awareness and attitudes of primary healthcare providers. Furthermore, it can be used in health and treatment policy-making as a basis for assessing educational needs and designing training courses.25,26
This study had several limitations that should be considered when interpreting the findings. First, the sample consisted of a specific group of healthcare providers from East Azerbaijan province, which may limit the generalizability of the results to other regions or to different professional groups, such as specialist physicians. Future psychometric studies in other parts of the country are recommended to enhance external validity. Additionally, while this study evaluated the instrument’s validity and reliability using CFA and Cronbach’s alpha, employing other methods such as convergent and discriminant validity could further clarify the tool’s factor structure. Potential differences in attitudes and knowledge among other healthcare professional groups and across diverse cultural contexts within Iran also warrant further investigation, as such studies could help improve the generalizability of the results and support the development of more tailored educational interventions.
Furthermore, the expert panel in this study was primarily composed of psychiatrists, psychologists, and health education specialists, without including individuals with direct experience or lived expertise in transgender health or LGBTQ + issues. This limitation should be addressed in future research to enhance the content validity assessment. Lastly, although both forward translation and back-translation were conducted by professional translators, only one back-translator was used. Future studies are advised to engage multiple independent translators and incorporate pilot testing or cognitive interviews with the target population to improve the cultural validity of the instrument.
Study Highlights
What is current knowledge?
-
Gender dysphoria is a significant challenge in healthcare systems, and primary healthcare providers play a central role in identifying, referring, and supporting these individuals.
-
Inadequate knowledge and negative attitudes among providers can result in poor quality of care and limited access to appropriate services.
-
There is no standardized and validated Persian-language questionnaire to measure healthcare providers’ knowledge and attitudes toward gender dysphoria.
What is new here?
-
This study psychometrically evaluated a Persian version of the questionnaire assessing primary healthcare providers’ knowledge and attitudes toward gender dysphoria.
-
The tool demonstrated good validity (CVI = 0.81, CVR = 0.93) and reliability (Cronbach’s alpha = 0.86, ICC = 0.76).
-
Confirmatory factor analysis supported a two-factor structure (knowledge and attitude), with an acceptable model fit.
-
The questionnaire can now be applied as a reliable screening and evaluation instrument in educational, clinical, and policy-making contexts in Iran.
Conclusion
This study evaluated a tool for measuring the knowledge and attitudes of primary healthcare providers regarding gender dysphoria and showed that the designed questionnaire has good validity and reliability. The results of the CFA showed that the two-factor structure of the tool (knowledge and attitude sections) is a suitable fit. However, it is essential to emphasize that the knowledge subscale demonstrated lower factor loadings for several items and a borderline acceptable internal consistency (Cronbach’s alpha = 0.65), which may reflect some conceptual complexity and variability in knowledge among participants. This limitation should be taken into account when interpreting the results, and future research is recommended to refine the knowledge subscale to enhance its reliability and clarity. This questionnaire can be used as a valid tool for assessing and improving the awareness and attitudes of primary healthcare providers in the field of gender dysphoria and is helpful in designing educational and research programs in this field.
Competing Interests
The authors declare no conflicts of interest
Data Availability Statement
Data are available upon reasonable request from the corresponding author.
Ethical Approval
Approved by the Regional Ethics Committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1402.427), this study obtained written informed consent from participants, ensured no additional costs, guaranteed withdrawal rights, and adhered to the Helsinki Declaration.
Acknowledgements
The authors express gratitude to the East Azerbaijan Province Health Centers for their support.
References
- Garg G, Elshimy G, Marwaha R. Gender dysphoria. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025.
- Badiei D, Golparvar M, Aghaei A. Comparing the effectiveness of resilience training package and positive therapy on social stigma of mothers of people suffering from gender dysphoria disorder. Iranian Journal of Psychiatric Nursing 2022;10(4):53-64. [Persian].
- Ghazanfari F, Khodarahimi S. Gender dysphoria disorder: diagnosis, theory and intervention. Rooyesh 2018;6(4):9-28. [Persian].
- Rahimi Ahmadabadi S, Kalantari M, Abedi MR, Modares Gharavi M. Role of family function in the prediction of gender dysphoria in women and transgender men. Shenakht Journal of Psychology and Psychiatry 2021;8(1):38-47. [Persian].
- Shafiei Kandjani AR, Sadeghpour S, Samadirad B, Mehrara A, Hosseinnejad P, Shalchi B. Demographic characteristics and personality disorders in people with gender dysphoria in East Azerbaijan province, Iran. Int J Med Toxicol Forensic Med 2022; 12(2):e36056. doi: 10.32598/ijmtfm.v12i2.36056 [Crossref] [ Google Scholar]
- Sadock BJ, Sadock VA. Kaplan & Sadock’s Concise Textbook of Clinical Psychiatry. Lippincott Williams & Wilkins; 2008.
- Zucker KJ, Lawrence AA, Kreukels BP. Gender dysphoria in adults. Annu Rev Clin Psychol 2016; 12:217-47. doi: 10.1146/annurev-clinpsy-021815-093034 [Crossref] [ Google Scholar]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: APA; 2013.
- Danafar AA, Jahanbakhsh I, Behyan S. Gender identity disorder and its social consequences among transsexuals referred to the social welfare organization in 2013-2015. Iran Sociol Rev 2017; 7(4):27-35. [ Google Scholar]
- Safer JD, Coleman E, Feldman J, Garofalo R, Hembree W, Radix A. Barriers to healthcare for transgender individuals. Curr Opin Endocrinol Diabetes Obes 2016; 23(2):168-71. doi: 10.1097/med.0000000000000227 [Crossref] [ Google Scholar]
- Riggs DW, Bartholomaeus C. Australian mental health nurses and transgender clients: attitudes and knowledge. J Res Nurs 2016; 21(3):212-22. doi: 10.1177/1744987115624483 [Crossref] [ Google Scholar]
- Freeman R, Ismail A. Assessing patients’ health behaviours Essential steps for motivating patients to adopt and maintain behaviours conducive to oral health. Monogr Oral Sci 2009; 21:113-27. doi: 10.1159/000224216 [Crossref] [ Google Scholar]
- Shafiee-Kandjani AR, Azarmi L, Shalchi B, Malek A, Davtalab-Esmaeili E, Turan Ş. Mental health literacy among individuals with gender dysphoria and its correlations with satisfaction of basic psychological needs: a cross-sectional study in northwest of Iran. Transgend Health. 2025. doi: 10.1089/trgh.2024.0172.
- Lee SR, Kim MA, Choi MN, Park S, Cho J, Lee C. Attitudes toward transgender people among medical students in South Korea. Sex Med 2021; 9(1):100278. doi: 10.1016/j.esxm.2020.10.006 [Crossref] [ Google Scholar]
- Shafiee-Kandjani AR, Shalchi B, Raeisnia A, Tajlil S, Davtalab-Esmaeili E. The association between personality traits and transphobia among university students: a cross-sectional study in northwestern Iran. BMC Psychiatry 2025; 25(1):80. doi: 10.1186/s12888-025-06509-9 [Crossref] [ Google Scholar]
- Chisolm-Straker M, Jardine L, Bennouna C, Morency-Brassard N, Coy L, Egemba MO. Transgender and gender nonconforming in emergency departments: a qualitative report of patient experiences. Transgend Health 2017; 2(1):8-16. doi: 10.1089/trgh.2016.0026 [Crossref] [ Google Scholar]
- James S, Herman J, Rankin S, Keisling M, Mottet L, Anafi MA. The Report of the 2015 US Transgender Survey. National Center for Transgender Equality (NCTE); 2016.
- Walch SE, Ngamake ST, Francisco J, Stitt RL, Shingler KA. The attitudes toward transgendered individuals scale: psychometric properties. Arch Sex Behav 2012; 41(5):1283-91. doi: 10.1007/s10508-012-9995-6 [Crossref] [ Google Scholar]
- Chester SD, Ehrenfeld JM, Eckstrand KL. Results of an institutional LGBT climate survey at an academic medical center. LGBT Health 2014; 1(4):327-30. doi: 10.1089/lgbt.2013.0055 [Crossref] [ Google Scholar]
- Afrasiabifar A, Yaghmaei F, Abdoli S, Abedsaeedi Z. Research tool translation and cross-cultural adaptation. Adv Nurs Midwifery 2006;16(54):58-67. [Persian].
- Daniali S, Jokar AA, Razavi S, Sedaghatnia MH, Azmoodeh M, Kalani N. The effect of Jahrom nurses’ attitude on knowledge sharing in the acceptance of clinical information technology systems. Iran J Emerg Med 2022; 9(1):e38. doi: 10.22037/ijem.v9i1.39928 [Crossref] [ Google Scholar]
- Mahieu L, de Casterlé BD, Van Elssen K, Gastmans C. Nurses’ knowledge and attitudes towards aged sexuality: validity and internal consistency of the Dutch version of the Aging Sexual Knowledge and Attitudes Scale. J Adv Nurs 2013; 69(11):2584-96. doi: 10.1111/jan.12113 [Crossref] [ Google Scholar]
- Howard A, Michael PG. Psychometric properties and factor structure of the attitudes toward research scale in a graduate student sample. Psychol Learn Teach 2019; 18(3):259-74. doi: 10.1177/1475725719842695 [Crossref] [ Google Scholar]
- Muzaheed M, El-Masry OS, Rabaan AA, Alzahrani F, Alomar A, Farooqi FA. Comparative cross-sectional assessment of knowledge, attitude and practice among university students and employees towards the use of the microbiology laboratory equipment. F1000Res 2021; 10:117. doi: 10.12688/f1000research.49923.2 [Crossref] [ Google Scholar]
- Budge SL, Adelson JL, Howard KA. Anxiety and depression in transgender individuals: the roles of transition status, loss, social support, and coping. J Consult Clin Psychol 2013; 81(3):545-57. doi: 10.1037/a0031774 [Crossref] [ Google Scholar]
- Rowan SP, Lilly CL, Shapiro RE, Kidd KM, Elmo RM, Altobello RA. Knowledge and attitudes of health care providers toward transgender patients within a rural tertiary care center. Transgend Health 2019; 4(1):24-34. doi: 10.1089/trgh.2018.0050 [Crossref] [ Google Scholar]
- Shafiee-Kandjani AR, Tajlil S, Raeisnia A, Turan Ş, Shalchi B. Psychometric properties of the genderism and transphobia scale in Iranian students. Health Promot Perspect 2025; 15(1):73-81. doi: 10.34172/hpp.025.43507 [Crossref] [ Google Scholar]