J Res Clin Med. 13:35141.
doi: 10.34172/jrcm.025.35141
Original Article
The predictive value of the SMART-COP score in the management of acute pulmonary embolism in the emergency department
Fatma Tortum Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing, 1, * 
Erdal Tekin Conceptualization, Formal analysis, Investigation, Project administration, Software, Validation, Writing – original draft, Writing – review & editing, 1
Bugra Kerget Data curation, Formal analysis, Methodology, Software, Writing – review & editing, 2
Alperen Aksakal Funding acquisition, Resources, Supervision, Visualization, Writing – review & editing, 2
Ozcan Agyurek Data curation, Investigation, Resources, Supervision, Visualization, Writing – review & editing, 1
Author information:
1Department of Emergency Medicine, School of Medicine, Ataturk University, Erzurum, Turkey
2Department of Pulmonary Diseases, School of Medicine, Ataturk University, Erzurum, Turkey
Abstract
Introduction:
The current study evaluates how well the SMART-COP score predicts the necessity for hospitalization in patients diagnosed with acute pulmonary embolism (APE) within the emergency department (ED).
Methods:
A prospective study was conducted between July 10, 2023, and March 10, 2024, in the ED of a tertiary care hospital and included 105 patients diagnosed with APE. The echocardiographic findings along with the clinical outcomes of the patients in the ED (hospitalization or discharge) were correlated with the SMART-COP score. Statistical analyses were conducted utilizing SPSS version 25 (IBM Corp., Armonk, NY). To assess the predictive power of the SMART-COP score in determining the need for hospitalization, receiver operating characteristic (ROC) analysis was undertaken.
Results:
The study found that patients requiring hospitalization had higher SMART-COP scores, which were positively associated with right ventricular (RV) dysfunction and elevated pulmonary artery pressure (PAP). The SMART-COP score demonstrated a cut-off value of 2.50, with sensitivity and specificity values of 85.1% and 71.1%, respectively.
Conclusion:
The findings suggest that the SMART-COP score may serve as a valuable tool for assessing the need for hospitalization in patients with APE within the ED setting. This study highlights the importance of the SMART-COP score in the management of APE, particularly along with hemodynamic instability criteria. Also, this paper introduces the clinical application of SMART-COP score in rapid and efficient evaluations in emergency care.
Keywords: Emergency department, Medicine, Pulmonary embolism, Vital sign
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
None.
Introduction
The increased clinical suspicion and growing use of diagnostic imaging have led to a higher incidence of acute pulmonary embolism (APE) diagnoses in emergency departments (ED). However, asymptomatic cases of APE are often detected incidentally during the emergency settings,1 but, a recent research indicated pulmonary embolism (PE) as the third leading cause of death worldwide.2
According to severity of the disease, APE is classified into massive/high-risk, submassive/intermediate-risk, and small/low-risk PE, which is determined not by the size of the embolus, but by the patient’s hemodynamic stability. The hemodynamic instability is typically defined as a systolic blood pressure (SBP) less than 90 mm Hg.3 Among the hemodynamically stable patients, submassive/intermediate-risk and small/low-risk PE cases are differentiated based on the presence or absence of right ventricular (RV) strain on computed tomography (CT), echocardiography, or elevated cardiac troponins.3
After a patient diagnosed as APE, a prompt identification of massive and submassive cases is crucial to ensure the appropriate hospitalization and to get the access to thrombolytic therapy, which can significantly reduce the risk of mortality. This decision-making process often relies on parameters such as blood pressure, increased right heart pressures on echocardiography, pulmonary angiography, and biomarkers of cardiac injury, all of which indicate RV overload. Since most of the mentioned assessments are necessitated to be performed by a specialist, like a radiologist or a cardiologist, Then, there is ongoing research to develop simpler clinical risk scoring systems to facilitate the primary evaluations.
The SMART-COP score was originally developed as a clinical tool for assessing the severity of pneumonia and determining the need for vasopressor support. This risk score is calculated by assigning points for the following criteria: SBP < 90 mm Hg, the presence of multilobar involvement on chest X-ray, albumin level < 35 g/L, increased respiratory rate (RR), tachycardia ( ≥ 125 beats/min), altered mental status (confusion), low oxygen levels, and arterial blood gas pH < 7.35.4
Since the parameters included in SMART-COP score are easily reachable in the ED thus, we aimed to determine whether the SMART-COP score could be effectively used to assess the hospitalization requirements for patients with APE, or not.
Materials and Methods
Study design
This prospective study involved the patients with APE in the ED of a tertiary care facility between the July 10, 2023 and March 10, 2024. Ethical approval was granted by the Clinical Research Ethics Committee of Ataturk University Faculty of Medicine. Participants were fully informed about the study, and their written consent was obtained. The research adhered to the principles outlined in the Declaration of Helsinki, Finland.
Study population
The current study included patients over 18 years old, which were diagnosed with APE in the ED. The patients who did not consent to participate, and those with chronic respiratory diseases, that could chronically elevate RV pressure (such as chronic obstructive pulmonary disease), pulmonary hypertension, acute or chronic renal failure, unable to undergo pulmonary angiography, for any reason, patients with incomplete data, pregnant patients, and those who left the hospital without permission during their treatment, were excluded from the study. During the study period, 231 patients were diagnosed with APE in the ED, among which 23 had poor pulmonary angiography images, 18 were transferred to another facility, 31 had unavailable echocardiographic findings at the time of admission, 12 declined to participate, 32 had incomplete vital data, and 10 had unavailable X-ray images. After excluding these patients, the final sample consisted of 105 APE patients.
Data collection
For each patient, demographic and clinical data including age, gender, SBP, diastolic blood pressure (DBP), RR, heart rate, oxygen saturation, and the presence of confusion were recorded at the time of admission,. These data were collected by an emergency medicine resident who was blinded to the study. Blood gas analyses, including pH and oxygen levels, were obtained from radial artery samples using a heparinized syringe and recorded in the study files by the same physician. The albumin levels measured in venous blood samples taken at the time of the admission, along with the presence of multilobar infiltrates on chest X-rays, were also recorded in the study files. Using this information, the total SMART-COP score for each patient was calculated and documented.
Moreover, D-dimer and troponin levels were measured at the time of admission. Echocardiographic findings, including pulmonary artery pressure (PAP), RV and/or atrial dilation, RV free wall hypokinesia, McConnell’s sign, interventricular septal flattening (“D-shaped” sign), dilated inferior vena cava, the presence of thrombi in the right heart, and ejection fraction, were recorded by a cardiologist with five years of experience. After evaluation by a pulmonologist, the patient’s final outcome in the ED, whether they were discharged or hospitalized, and whether thrombolytic therapy was administered or not were also noted. All records were transferred to an electronic database.
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY). The Kolmogorov-Smirnov test was used to assess normality. Descriptive statistics were presented as frequencies and percentages for categorical variables and as means with standard errors for continuous variables. chi-square and Fisher’s exact tests and Mann-Whitney U test were used to compare the categorical and non-normally distributed variables, respectively. Spearman’s correlation analysis was performed to examine the relationships between non-normally distributed variables.
Receiver operating characteristic (ROC) analysis was conducted to evaluate the predictive power of the SMART-COP score in determining hospitalization versus discharge in patients with APE. The area under the ROC curve (AUC) was calculated for PAP, RV involvement, and the SMART-COP score. The Youden J index was used to determine the optimal cut-off values. Sensitivity and specificity were calculated with 95% confidence intervals (CIs). A P value of less than 0.05 was considered as statistically significant.
Results
The study included a total of 105 patients, of whom 67 were hospitalized. The mean age of the patients was 68.4 ± 12.3 years, and 50.5% (n = 53) were male. When comparing patients discharged from the ED with those who were hospitalized, it was found that heart rate, RR, troponin, D-dimer, PAP, RV involvement, and SMART-COP scores were significantly higher in hospitalized patients, while oxygen saturation was significantly lower for them (P < 0.05 for all). Table 1 presents the baseline characteristics of patients according to their outcome in the ED.
Table 1.
Baseline characteristics of patients according to their outcome in the emergency department
|
|
Total (n=105)
|
Discharged (n=38)
|
Hospitalized (n=67)
|
P
value
|
| Age, year |
68.4 ± 12.3 |
68.1 ± 12.4 |
68.6 ± 12.3 |
0.886 |
| Gander, male |
53 (50.5%) |
22 (57.9%) |
31 (46.3%) |
0.254 |
| SBP, mm Hg |
121.0 ± 23.5 |
122.1 ± 12.3 |
120.4 ± 28.0 |
0.810 |
| DBP, mm Hg |
73.6 ± 14.8 |
73.3 ± 7.9 |
73.7 ± 17.6 |
0.426 |
| Heart rate, /min |
103.8 ± 21.8 |
95.6 ± 18.1 |
108.5 ± 22.4 |
0.005 |
| Saturation, % |
82.9 ± 7.6 |
86.2 ± 7.2 |
81.0 ± 7.2 |
0.001 |
| Respiratory rate, /min |
20.2 ± 5.4 |
18.4 ± 4.1 |
21.2 ± 5.7 |
0.011 |
| Albumin, g/dL |
5.7 ± 21.7 |
3.6 ± 0.5 |
6.9 ± 27.2 |
0.942 |
| Troponin, pg/mL |
243.4 ± 1411.7 |
51.7 ± 114.0 |
352.1 ± 1760.7 |
< 0.001 |
| D-dimer, g/mL |
9,002.5 ± 9,747.7 |
6,172.2 ± 9,181.8 |
10,607.7 ± 9,758.9 |
< 0.001 |
| Ph |
7.43 ± 0.05 |
7.43 ± 0.04 |
7.43 ± 0.06 |
0.981 |
| Chest X-ray findings |
54 (51.4%) |
17 (44.7%) |
37 (55.2%) |
0.568 |
| Ejection fraction, % |
54.0 ± 3.5 |
54.5 ± 1.6 |
53.7 ± 4.2 |
0.752 |
| PAP, mm Hg |
44.6 ± 15.6 |
36.3 ± 11.1 |
49.3 ± 15.8 |
< 0.001 |
| RVI |
45 (42.9%) |
3 (7.9%) |
42 (62.7%) |
< 0.001 |
| SMART-COP score |
3.3 ± 2.0 |
1.8 ± 1.2 |
4.2 ± 1.9 |
< 0.001 |
| Thrombolytic therapy |
30 (28.6%) |
0 (0%) |
30 (44.8%) |
< 0.001 |
| Mortality |
16 (15.2%) |
4 (10.5%) |
12 (17.9%) |
0.119 |
Note: SBP: Systolic blood pressure; DBP: Diastolic blood pressure; PAP: Pulmonary artery pressure; RVI: Right ventricular involvement
Table 2 presents the correlation of SMART-COP scores with other variables. Accordingly, the SMART-COP score was negatively correlated with SBP, DBP, oxygen saturation, pH, and ejection fraction, all of which were statistically significant (P < 0.05). Positive and statistically significant correlations were observed between the SMART-COP score and the remaining parameters (P < 0.05).
Table 2.
Correlation of the SMART-COP score with other variables
|
SMART-COP score
|
SBP
|
DBP
|
HR
|
Sat
|
RR
|
Al
|
pH
|
EF
|
PAP
|
RVI
|
TT
|
ED
|
|
r
|
-0.494 |
-0.409 |
0.486 |
-0.564 |
0.505 |
0.218 |
-0.213 |
-0.193 |
0.418 |
0.586 |
0.712 |
0.546 |
|
P
|
< 0.001 |
< 0.001 |
< 0.001 |
< 0.001 |
< 0.001 |
0.026 |
0.029 |
0.049 |
< 0.001 |
< 0.001 |
< 0.001 |
< 0.001 |
Note: SBP: Systolic blood pressure; DBP: Diastolic blood pressure; HR: Heart rate; Sat: Saturation; RR: Respiratory rate; Al: Albumin;EF; Ejection fraction; PAP: Pulmonary artery pressure; RVI: Right ventricular involvement; TT: Thrombolytic therapy; ED: Emergency decision
The ROC analysis revealed that the AUC values of PAP, RV involvement, and SMART-COP score in predicting the need for hospitalization in the ED were 0.757, 0.774, and 0.846, respectively (P < 0.001). At a cut-off value of 2.50, the SMART-COP score showed a sensitivity of 85.1% and a specificity of 71.1% (AUC = 0.846, P < 0.001) (Figure 1, Table 3).
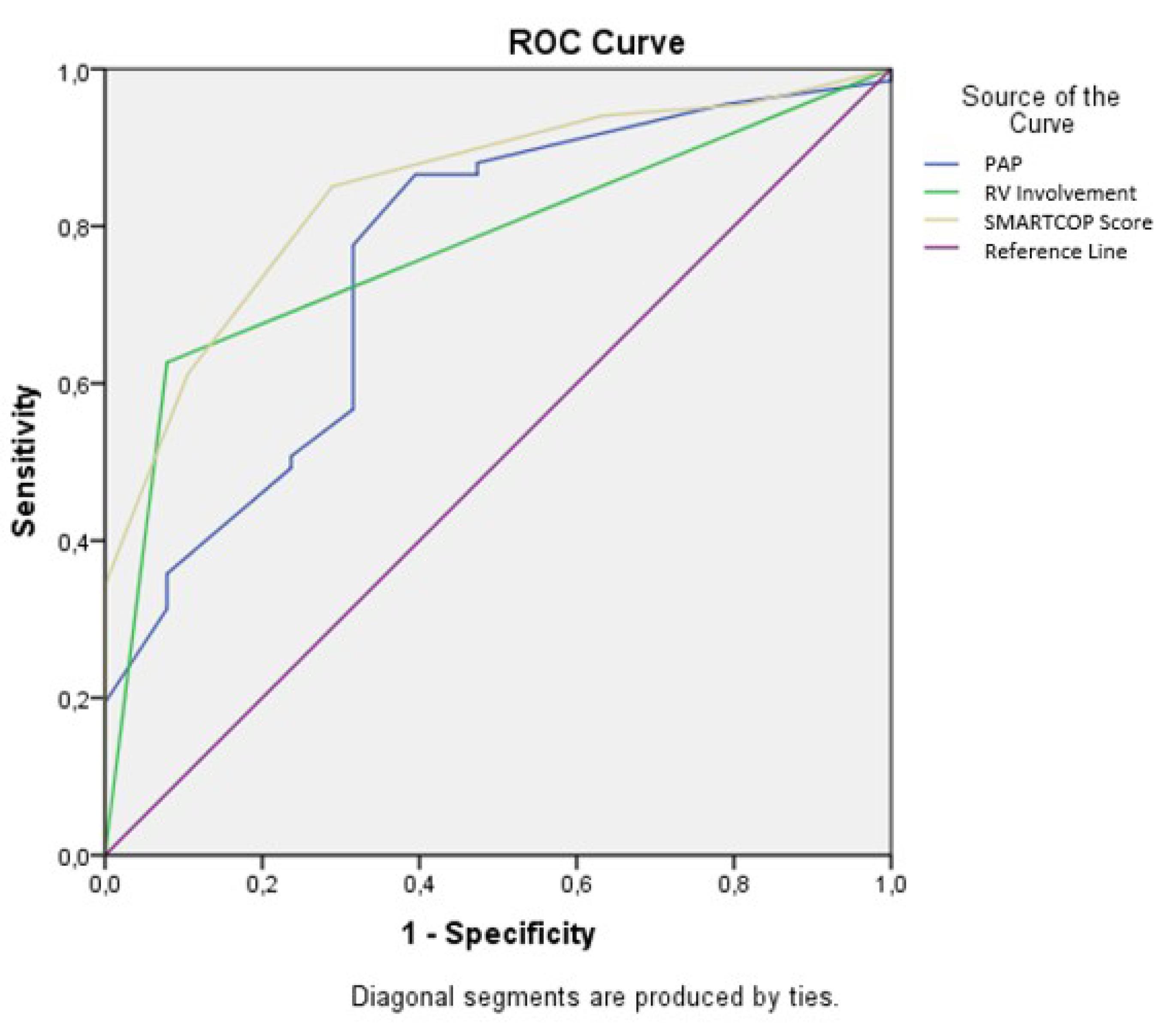
Figure 1.
Receiver operating characteristic curve (ROC) for predicting hospitalization in patients diagnosed with acute pulmonary embolism in the emergency department
.
Receiver operating characteristic curve (ROC) for predicting hospitalization in patients diagnosed with acute pulmonary embolism in the emergency department
Table 3.
Performance of the investigated variables for predicting hospitalization in patients diagnosed with acute pulmonary embolism in the emergency department
|
Variables
|
Cut-off
|
AUC
|
SE
|
Sensitivity (%)
|
Specificity (%)
|
95% CI
|
P
value
|
| PAP |
> 36.0 |
0.757 |
0.050 |
0.776 |
0.684 |
0.660–0.854 |
< 0.001 |
| RVI |
> 0.50 |
0.774 |
0.046 |
0.627 |
0.921 |
0.684–0.864 |
< 0.001 |
| SMART-COP score |
> 2.50 |
0.846 |
0.038 |
0.851 |
0.711 |
0.772–0.920 |
< 0.001 |
Note: AUC: Area under the curve; SE: Standard error; CI: Confidence interval; PAP: Pulmonary artery pressure; RVI: Right ventricular involvement
Discussion
The current study is the very first published study examining the relationship between the SMART-COP score and APE status. The observations indicated a positive correlation between the SMART-COP score and the need for hospitalization, RV involvement, and PAP values for patients diagnosed with APE in the ED. Patients with higher SMART-COP scores had a higher probability of being hospitalized compared to those with lower scores. A SMART-COP cut-off value of 2.50 had a sensitivity of 85.1% and a specificity of 71.1% to predict the hospitalization for these patients. In addition, as the SMART-COP score increased, PAP and RV involvement also increased.
The components of the SMART-COP scoring system, such as systolic hypotension, tachycardia, hypoxia, increased RR due to hypoxia, and the confusion related to severe hypoxia, may be helpful in determining the need for hospitalization and thrombolytic therapy in patients with APE. Many of these parameters are also a part of the widely accepted PE severity index (PESI).5 However, the albumin parameter included in the SMART-COP scoring system is not presented in the PESI, which allows the SMART-COP score to provide a broader perspective.
Studying the pathophysiology of APE, it is understood that ventilation/perfusion mismatch results in hypoxia6 which results in RR increases. These are reflected in SMART-COP scoring system as 2 points for hypoxia and 1 point for increased RR. Although hypoxia and tachypnea are not considered as a hemodynamic instability criterion, but they are common findings in patients with APE. Furthermore, hypoxia can contribute to altered mental status in these patients. Although hypoxia alone is not used as a criterion for hemodynamic instability, its consequence, i.e., confusion, is assigned 1 point in the SMART-COP scoring system. Furthermore, the thrombus-induced vasospasm causing hemodynamic instability in patients with APE is located in the pulmonary artery. The primary treatment for thrombi that cause hemodynamic instability is thrombolytic therapy. An SBP level less than 90 mm Hg is assigned 2 points in SMART-COP score and it is also considered as a criterion for hemodynamic instability in APE.7 Additionally, the tachycardia, resulted by hypotension and hypoxia, which has 1 point in the SMART-COP scoring system is a criterion for instability,8 can also be considered a Therefore, the inclusion of systolic hypotension, tachycardia, and altered mental state, which are key indicators of hemodynamic instability in APE, within the SMART-COP score suggests that it can be useful in distinguishing patients requiring hospitalization and thrombolytic therapy.
Albumin is frequently used in the ED as both a negative acute-phase reactant and an indicator of nutritional status. It is also known for its antioxidant, anti-inflammatory, and anticoagulant properties and its positive role in maintaining microvascular integrity.9 Due to these functions, albumin has been the subject of many studies related to venous thrombosis. Observations have indicated that the risk of venous thrombosis increases in patients with hypoalbuminemia.10-12 Considering the relationship between hypoalbuminemia and thrombosis, the inclusion of albumin levels in the SMART-COP score differentiates it from the PESI. In a study evaluating mortality in APE cases with hypoalbuminemia, it was observed that APE was more fatal in patients with low albumin levels.11,13 Therefore, incorporating albumin into scoring systems that assess both diagnosis and prognosis could be a rational approach.
Chest X-ray imaging reveals various abnormalities in patients with APE. In one study, the rate of consolidation on chest X-rays in patients with APE was found to be 25%.14 Multilobar consolidation on chest X-ray is another parameter included in the SMART-COP scoring system. Although pulmonary angiography is considered as the gold standard for diagnosis, it has some limitations, such as the risk of contrast allergy, contrast-induced nephropathy, and restricted access to radiology services.15 Given its lower cost and faster evaluation, a chest X-ray may be considered as an initial imaging tool in suspected APE cases in the ED.
In APE, an increase of PAP and RV involvement is expected. A related study demonstrated that there is a correlation between the degree of obstruction and the increase in PAP.16 An APE event, characterized by embolic obstruction in the pulmonary circulation affecting more than 30% of the vascular system, results in heightened pulmonary vascular resistance and the development of acute pulmonary arterial hypertension. This pulmonary vascular obstruction is further exacerbated by the release of vasoactive agents from plasma, platelets, or tissue, as well as reflex pulmonary arterial vasoconstriction, ultimately causing systemic arterial hypotension.17 This could explain why, in our study, the SMART-COP score was found to be associated not only with the need for hospitalization and thrombolytic therapy but also with elevated PAP levels.
Limitations
This research was carried out in an individual healthcare center with a relatively small patient population. Additionally, the studied patients were not categorized based on the clinical severity of APE. Furthermore, the study only evaluated the ability of the SMART-COP score to predict hospitalization at the time of ED years presentation without exploring the relationship between this score and mortality.
Study Highlights
What is current knowledge?
What is new here?
-
SMART-COP score is a valuable tool for assessing the severity of acute pulmonary embolism (APE) and is correlated with clinical outcomes such as the need for hospitalization, right ventricular dysfunction, and elevated pulmonary artery pressure.
Conclusion
The SMART-COP scoring system was found to be highly effective in predicting hospitalization in patients with APE. The correlation of the SMART-COP score with RV involvement and PAP suggests that this score may be useful for predicting hospitalization.
As a simple and practical scoring tool for use in the ED, the SMART-COP score may not be the sole criterion for determining hospitalization but can guide clinicians in identifying patients who require further evaluation and intervention.
Competing Interests
The authors declare no conflict of interest.
Ethical Approval
Ethical approval was obtained from the Clinical Research Ethics Committee of the Ataturk University Faculty of Medicine (meeting date: July 6, 2023; decision number: 5/29). Informed consent was obtained from the patients.
References
- Gönen B, Hanci P, Hatipoğlu ON. Characteristics of patients with symptomatic and incidental pulmonary thromboembolism. Tuberk Toraks 2024; 72(3):179-84. doi: 10.5578/tt.202403946 [Crossref] [ Google Scholar]
- Martinez Licha CR, McCurdy CM, Maldonado SM, Lee LS. Current management of acute pulmonary embolism. Ann Thorac Cardiovasc Surg 2020; 26(2):65-71. doi: 10.5761/atcs.ra.19-00158 [Crossref] [ Google Scholar]
- Trott T, Bowman J. Diagnosis and management of pulmonary embolism. Emerg Med Clin North Am 2022; 40(3):565-81. doi: 10.1016/j.emc.2022.05.008 [Crossref] [ Google Scholar]
- Tsai D, Secombe P, Chiong F, Ullah S, Lipman J, Hewagama S. Prediction accuracy of commonly used pneumonia severity scores in Aboriginal patients with severe community-acquired pneumonia: a retrospective study. Intern Med J 2023; 53(1):51-60. doi: 10.1111/imj.15534 [Crossref] [ Google Scholar]
- Howard L. Acute pulmonary embolism. Clin Med (Lond) 2019; 19(3):243-7. doi: 10.7861/clinmedicine.19-3-247 [Crossref] [ Google Scholar]
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J 2020; 41(4):543-603. doi: 10.1093/eurheartj/ehz405 [Crossref] [ Google Scholar]
- Zuo Z, Yue J, Dong BR, Wu T, Liu GJ, Hao Q. Thrombolytic therapy for pulmonary embolism. Cochrane Database Syst Rev 2021; 4(4):CD004437. doi: 10.1002/14651858.CD004437.pub6 [Crossref] [ Google Scholar]
- Götzinger F, Lauder L, Sharp AS, Lang IM, Rosenkranz S, Konstantinides S. Interventional therapies for pulmonary embolism. Nat Rev Cardiol 2023; 20(10):670-84. doi: 10.1038/s41569-023-00876-0 [Crossref] [ Google Scholar]
- Abedi F, Zarei B, Elyasi S. Albumin: a comprehensive review and practical guideline for clinical use. Eur J Clin Pharmacol 2024; 80(8):1151-69. doi: 10.1007/s00228-024-03664-y [Crossref] [ Google Scholar]
- Hoseiny Nejad N, Sharif AS, Otukesh H, Hosseini Shamsabadi R, Hekmat S, Sakhaei M. Determination of the value of albumin, anti-thrombin III, fibrinogen and D-dimer factors in the diagnosis of asymptomatic pulmonary embolism in patients with nephrotic syndrome. Pediatr Nephrol 2021; 36(7):1803-8. doi: 10.1007/s00467-020-04904-w [Crossref] [ Google Scholar]
- Özcan S, Dönmez E, Yavuz Tuğrul S, Şahin İ, İnce O, Ziyrek M. The prognostic value of C-reactive protein/albumin ratio in acute pulmonary embolism. Rev Invest Clin 2022; 74(2):097-103. doi: 10.24875/ric.21000547 [Crossref] [ Google Scholar]
- Valeriani E, Pannunzio A, Palumbo IM, Bartimoccia S, Cammisotto V, Castellani V. Risk of venous thromboembolism and arterial events in patients with hypoalbuminemia: a comprehensive meta-analysis of more than 2 million patients. J Thromb Haemost 2024; 22(10):2823-33. doi: 10.1016/j.jtha.2024.06.018 [Crossref] [ Google Scholar]
- Elshahaat HA, Zayed NE, Ateya MA, Safwat M, El Hawary AT, Abozaid MN. Role of serum biomarkers in predicting management strategies for acute pulmonary embolism. Heliyon 2023; 9(11):e21068. doi: 10.1016/j.heliyon.2023.e21068 [Crossref] [ Google Scholar]
- Conrad TJ, Lau HX, Yerkovich ST, Alghamry A, Lee JC. Ventilation-perfusion scan for diagnosing pulmonary embolism: do chest X-rays matter?. Nucl Med Commun 2024; 45(3):181-7. doi: 10.1097/mnm.0000000000001802 [Crossref] [ Google Scholar]
- Kruger PC, Eikelboom JW, Douketis JD, Hankey GJ. Pulmonary embolism: update on diagnosis and management. Med J Aust 2019; 211(2):82-7. doi: 10.5694/mja2.50233 [Crossref] [ Google Scholar]
- Hajiahmadi S, Tabesh F, Shayganfar A, Shirani F, Ebrahimian S. Pulmonary artery obstruction index, pulmonary artery diameter and right ventricle strain as prognostic CT findings in patient with acute pulmonary embolism. Radiologia (Engl Ed) 2023; 65(3):200-12. doi: 10.1016/j.rxeng.2021.04.001 [Crossref] [ Google Scholar]
- An J, Nam Y, Cho H, Chang J, Kim DK, Lee KS. Acute pulmonary embolism and chronic thromboembolic pulmonary hypertension: clinical and serial CT pulmonary angiographic features. J Korean Med Sci 2022; 37(10):e76. doi: 10.3346/jkms.2022.37.e76 [Crossref] [ Google Scholar]