J Res Clin Med. 13:34938.
doi: 10.34172/jrcm.025.34938
Original Article
The prevalence and risk factors of fluoroquinolones and co-trimoxazole resistant Escherichia coli in the Northwest Iran: A retrospective cohort
Reyhaneh Ravanbakhsh Data curation, Formal analysis, Software, Visualization, Writing – review & editing, 1 
Mojtaba Varshochi Conceptualization, Supervision, Validation, 2, 3
Behrooz Naghili Conceptualization, Methodology, Writing – original draft, 2, 3
Alka Hasani Methodology, Writing – review & editing, 3, 4
Parinaz Poorshahverdi Writing – review & editing, 2
Ahad Bazmani Investigation, Writing – original draft, Writing – review & editing, 3
Fatemeh Ravanbakhsh Ghavghani Conceptualization, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing, 2, 3, *
Author information:
1Department of Aquatic Biotechnology, Artemia and Aquaculture Research Institute, Urmia University, Urmia, Iran
2Department of Infectious Diseases, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
3Infectious and Tropical Diseases Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
4Clinical Research Development Unit, Sina Educational, Research and Treatment Center, and Department of Medical Microbiology, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
Fluoroquinolone (FQ) and co-trimoxazole (STX) are the most effective antibiotics for Escherichia coli; however, antibiotic resistance has become an ever-increasing challenge. The current study investigates the prevalence rate and risk factors for developing FQ and STX resistance in Northwest Iran.
Methods:
This is a retrospective cohort study of 314 patients admitted to Sina Hospital, the academic hospital affiliated with Tabriz University of Medical Sciences, Iran, between 21st March 2017 to 20th March 2018. Based on specimen culture, patients were divided into two groups, i.e., FQ or SXT-resistant E. coli and the antibiotics sensitive. The potential risk factors for developing FQ or SXT-resistant E. coli were studied in the included patients.
Results:
FQ and SXT-resistant E. coli prevalence was 66.3% and 70%, respectively. Univariate analyses showed that type II diabetes mellitus, prior antibiotic use, prior FQ administration, prior admission, prior urinary tract infection, urinary catheterization, and anemia were the significant risk factors for developing FQ-resistant E. coli infection. The univariate analyses indicated that prior antibiotic use, hospitalization in an intensive care unit (ICU), and urinary catheterization were the significant risk factors for developing SXT-resistant E. coli infection. FQ and SXT-resistant E. coli infections are prevalent in our region. Prior antibiotic use and urinary catheterization are the common risk factors for developing FQ and SXT-resistant E. coli in our region.
Conclusion:
Type II diabetes mellitus, prior urinary tract infection, gentamicin resistance, prior FQ administration, and extended-spectrum β-lactamases (ESBL) production are risk factors for developing FQ-resistant E. coli and ESBL production is the risk factor for developing STX-resistant E. coli in our region.
Keywords: Escherichia coli, Fluoroquinolones, Microbial drug resistance, Trimethoprim sulfamethoxazole drug combination
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
Escherichia coli, the most common pathogen of the Enterobacteriaceae family, accounts for common clinical infections. Following antibiotic resistance, E. coli has become a significant public health challenge.1-3 Co-trimoxazole (SXT) and fluoroquinolones (FQs) are commonly administered antibiotics to treat infections mediated by E. coli. These antibiotics have been the first line of empiric therapy, especially in urinary tract infections; however, antibiotic resistance mechanisms have resulted in the development of FQ and SXT-resistant E. coli in clinical settings.4-7 Resistance to SXT has been increasingly reported among all E. coli strains isolated from community-acquired and nosocomial infections.2 Resistance to SXT appeared soon after its use was initiated in patients; the SXT-resistance rate was < 1% in early 1970 for E. coli strains from the urinary tract,8 while this number was reported at 84.4% for E. coli isolated from urine and wound specimens in 2012.9 In 2014-2018, 62.5% of uropathogenic E. coli was resistant to STX.10 In the United States, the SXT resistance rate varies from 20% to 25%.2 In a systematic review conducted in Iran on studies published from 1992 to 2015, the prevalence of SXT resistance in uropathogenic E. coli isolates was 62%.11 Therefore, its use in urinary tract infections as an empirical therapy has been restricted.2,7,12 Following the worrisome increase of SXT-resistant E. coli, FQs were considered as the first line of treatment agents; however, the excessive use of FQs has also led to FQ-resistance development in recent years.2,13 The prevalence of FQ-resistant E. coli in the USA and Europe was below 10%14 and 15.8%,15 respectively. Our previous research on uropathogenic E. coli isolates indicated that 54% were ciprofloxacin resistant.16
Although early reports of FQ and SXT resistance in E. coli suggested an association between FQ and SXT resistance,17 little consensus is present on the factors that enhance the risk of FQ and SXT-resistant infections. Few studies highlighted different risk factors for SXT or FQ-resistant E. coli.1,8,18-23 For SXT, recent hospitalization, the use of SXT,8 and recurrent urinary tract infection 23 have been listed as the risk factors. The risk factors for FQ-resistant development include older age, urinary catheterization,21 immunosuppression, previous infection,1 aminoglycoside use,24 antimicrobial therapy, and urinary tract infection.1 However, the prevalence and antimicrobial resistance patterns vary among different geographical regions; understanding the risk factors of antimicrobial resistance is crucial for identifying the high-risk groups.25 Therefore, the present study aimed to investigate the prevalence rate of FQ and SXT-resistant in E. coli isolates and risk factors for developing resistance to FQ and SXT in hospitalized patients in Northwest Iran.
Methods
This is a retrospective cohort study of 314 patients admitted to Sina Hospital, the academic hospital affiliated with Tabriz University of Medical Sciences, Iran, between 21st March 2017 to 20th March 2018. Following the study of microbiological reports, all patients with a positive culture of E. coli were selected for further analysis. These E. coli isolates were isolated from community-acquired or nosocomial infections. Identification of E. coli was performed using standard bacteriological techniques.26,27 The antimicrobial susceptibility testing was performed, and results were interpreted as described by the Clinical Laboratory Standard Institute (CLSI).27 E. coli isolates demonstrating FQ and/or SXT-resistance were considered as the case, and sensitive ones as the control group. Each patient was included as a case or control only once. If E. coli culture was positive on multiple occasions, only the first episode of infection was considered.
The medical records of included patients were reviewed to extract age, sex, source of infection, presence of an urinary catheter, history of smoking, nephrolithiasis, type II diabetes mellitus, hypertension, ischemic heart diseases, chronic renal failure, cancer, immunosuppressive therapy such as chemotherapy or corticosteroid therapy, benign prostatic hyperplasia, prior urinary tract infection, ICU admission, previous hospitalization in the last six months, prior FQ or SXT or another antibiotic use in the past 90 days, infecting with a nosocomial infection or colonization in the ICU, white blood cell count, hemoglobin, platelet, creatinine, erythrocyte sedimentation rates, procalcitonin, and antibiogram-based factors. This study was approved by the Ethics Committee of Tabriz University of Medical Sciences and the informed consent was obtained from the included patients. The protocol of this study is in line with the Helsinki Declaration of 1975, as revised in 2008 and is accordance with the ethical standards.
The obtained data were subjected to statistical analysis and represented as mean ± standard deviation (SD) and frequency (%). Univariate analysis was conducted to study the association between potential risk factors and FQ or SXT-resistant infection. All P-values were calculated using logistic regression. An odds ratio (OR) and 95% confidence interval (CI) were calculated to investigate any correlation between risk factors and FQ or SXT resistance. Adjusted ORs were calculated using unconditional logistic regression analysis with variables significance at a P value of ≤ 0.1, as assessed by univariate analysis, to control for all the confounding factors. Variables were included in the multivariate analysis in a stepwise manner to construct the final model. P values of less than 0.05 were considered as significant. SPSS v.22 was used for all statistical analysis.
Results
A total of 314 microbiologically confirmed E. coli isolates were collected from 173 women (55.1%) and 141 men (44.9%). The mean age of included patients was 64.1 years (range, 2 to 95 years). Forty-six (17.8%) of the included patients were hospitalized in the ICU, and 258 (82.2%) in non-ICU wards. The source of infection was asymptomatic and symptomatic urinary tract infection in 250 (79.6%) patients and the source of infection for the remaining patients was the bloodstream, respiratory, and wound site. In the urine isolates, 39.5% of patients had a urinary-catheter. The E. coli resistance rates to different antibiotics tested are depicted in Figure 1. Among the antibiotics investigated in the present study, the highest rates of resistance were observed for cefazolin (73.91%), cefotaxime (71.06%), co-trimoxazole (70%), ceftazidime (69.45%), fluoroquinolone (66.3%), gentamicin (33.55%), piperacillin-tazobactam (7.5%), nitrofurantoin (7.2%), amikacin (AN) (4.84%) and carbapenem (1.82%) (Figure 1). Among all E. coli isolates, 205 (65.3%) were extended-spectrum β-lactamases (ESBL) producing bacteria.
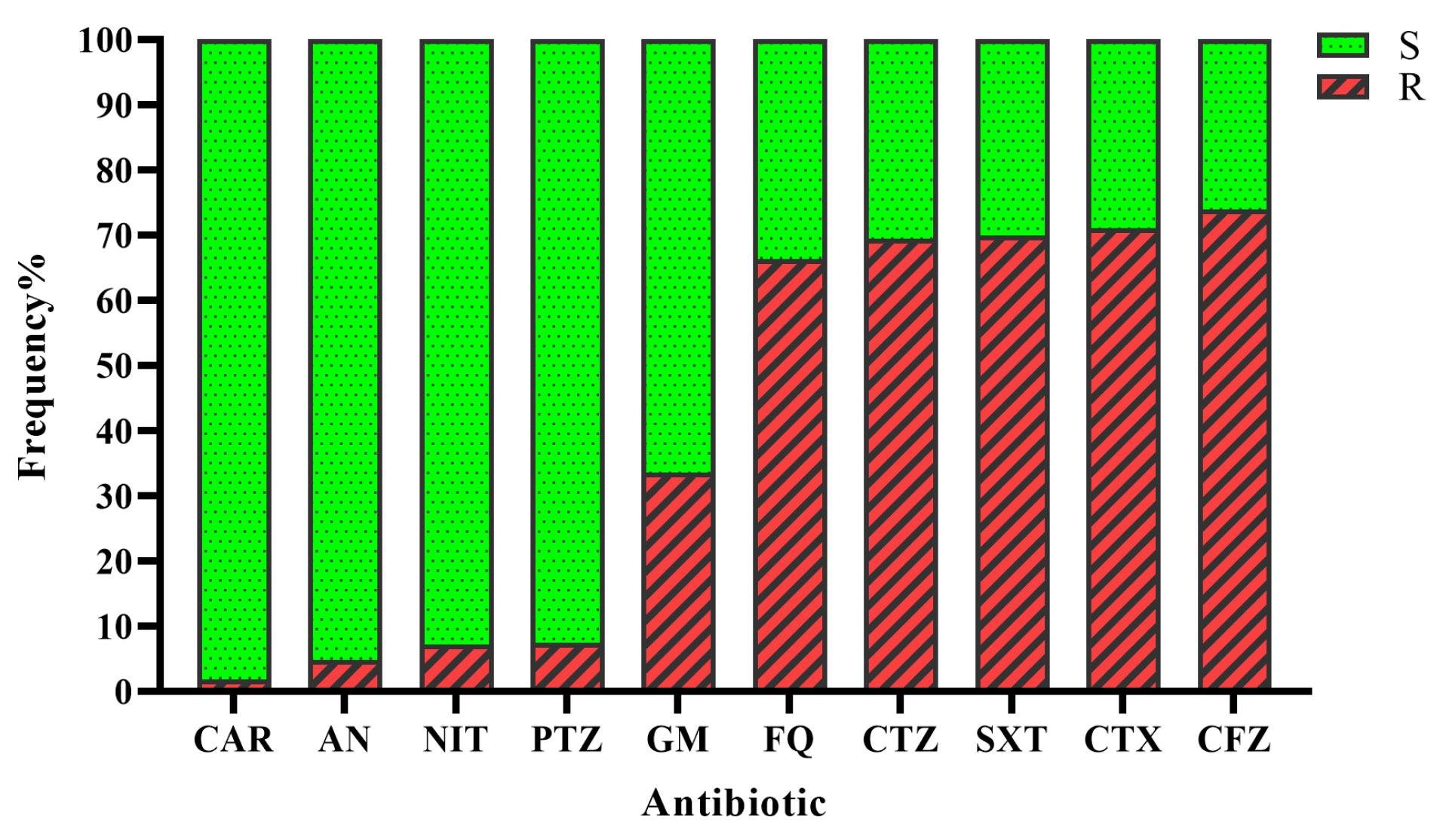
Figure 1.
Rates of resistance to different antibiotics tested against 314 E. coli strains isolated from urine, bloodstream, respiratory samples, and wounds. Abbreviations: CAR, carbapenem; AN, amikacin; NIT, nitrofurantoin; PTZ, piperacillin tazobactam; GM, gentamicin; FQ, fluoroquinolone; CTZ, ceftazidime; SXT, cotrimoxazole; CTX, cefotaxime; CFZ, cefazolin; S, sensitive strains; R, resistant strains
.
Rates of resistance to different antibiotics tested against 314 E. coli strains isolated from urine, bloodstream, respiratory samples, and wounds. Abbreviations: CAR, carbapenem; AN, amikacin; NIT, nitrofurantoin; PTZ, piperacillin tazobactam; GM, gentamicin; FQ, fluoroquinolone; CTZ, ceftazidime; SXT, cotrimoxazole; CTX, cefotaxime; CFZ, cefazolin; S, sensitive strains; R, resistant strains
FQ resistance
FQ resistance was observed in 66.3% of E. coli isolates. Among these, univariate analysis showed a history of type II diabetes mellitus (P value = 0.003, OR = 2. 1, 95% CI = 1.28-3.45), prior antibiotic administration (other than FQ and SXT) (P-value = 0.000, OR = 2.96, 95% CI = 1.75-5.1), prior FQ use (P value = 0.000, OR = 3.75, 95% CI = 1.82-7.71), prior admission (P value = 0.000, OR = 3.16, 95% CI = 1.77-5.65), prior urinary tract infection (P value = 0.005, OR = 5.59, 95% CI = 1.66-18.81), urinary catheterization (P value = 0.006, OR = 2.36, 95% CI = 1.28-4.34) (Table 1), anemia (P value = 0.006, OR = 2.16, 95% CI = 1.23-3.77) (Table 2), ESBL production (P value = 0.000, OR = 9.01, 95% CI = 5.23-15.53), gentamicin (P value = 0.000, OR = 11.69, 95% CI = 5.17-26.43) and SXT (P value = 0.000, OR = 2.98, 95% CI = 1.77-5.03) use (Table 3), were statistically significant risk factors associated with FQ resistance. It is worth mentioning that there was a trend toward significance for age > 65 years (P value = 0.068, OR = 1.56, 95% CI = 0.97-2.51) and hypertension history in patients (P value = 0.059, OR = 1.59, 95% CI -0.98-2.56) (Table 1).
Table 1.
Clinical factors associated with E. coli resistance to FQ and SXT as assessed by univariate analysis a
|
Risk Factors
|
Category
|
FQ OR (95% CI)
|
FQ
Pb value
|
SXT OR (95% CI)
|
SXT
Pb value
|
| Age |
<65 |
1 |
|
1 |
|
|
|
>65 |
1.56 (0.97-2.51) |
0.068
|
1.49 (0.91-2.44) |
0.118 |
| Sex |
Female |
1 |
|
1 |
|
|
|
Male |
1.23 (0.76-1.98) |
0.4 |
1.57 (0.946-2.607) |
0.081 |
| Smoking |
No |
1 |
|
1 |
|
|
|
Yes |
0.715 (0.39-1.3) |
0.27 |
1.105 (0.573-2.129) |
0.766 |
| Nephrolithiasis |
No |
1 |
|
1 |
|
|
|
Yes |
1.46 (0.75-2.85) |
0.26 |
1.199 (0.614-2.343) |
0.595 |
| DM |
No |
1 |
|
1 |
|
|
|
Yes |
2.1 (1.28-3.45) |
0.003
|
1.088 (0.66-1.792) |
0.741 |
| HTN |
No |
|
|
1 |
|
|
|
Yes |
1.59 (0.98-2.56) |
0.059 |
1.35 (0.82-2.22) |
0.237 |
| IHD |
No |
|
|
1 |
|
|
|
Yes |
1.25 (0.62-2.5) |
0.53 |
0.607 (0.31-1.184) |
0.143 |
| CRF |
No |
1 |
|
1 |
|
|
|
Yes |
1.37 (0.67-2.79) |
0.39 |
1.385 (0.648-2.96) |
0.4 |
| BPH |
No |
1 |
|
1 |
|
|
|
Yes |
1.91 (0.76-4.81) |
0.17 |
2.051 (0.722-5.83) |
0.178 |
| Cancer |
No |
1 |
|
1 |
|
|
|
Yes |
1.49 (0.69-3.2) |
0.31 |
1.13 (0.52-2.45) |
0.76 |
| ISD |
No |
1 |
|
1 |
|
|
|
Yes |
1.02 (0.47-2.19) |
0.97 |
0.573 (0.261-1.254) |
0.163 |
| Prior AB use |
No |
1 |
|
1 |
|
|
|
Yes |
2.96 (1.75-5.01) |
0.000
|
2.3 (1.34-3.92) |
0.002
|
| Prior FQ use |
No |
1 |
|
1 |
|
|
|
Yes |
3.75 (1.82-7.7) |
0.000
|
1.84 (0.96-3.53) |
0.065 |
| Prior SXT use |
No |
1 |
|
1 |
|
|
|
Yes |
0.50 (0.1-2.5) |
0.41 |
0.425 (0.059-3.07) |
0.4 |
| Prior admission |
No |
1 |
|
1 |
|
|
|
Yes |
3.16 (1.77-5.65) |
0.000
|
1.54 (0.89-2.66) |
0.12 |
| Prior UTI |
No |
1 |
|
1 |
|
|
|
Yes |
5.59 (1.66-18.81) |
0.005
|
1.61 (0.67-3.87) |
0.28 |
| ICU hospitalization |
No |
1 |
|
1 |
|
|
|
Yes |
0.79 (0.43-1.44) |
0.43 |
3.23 (1.41-7.48) |
0.004
|
| Uro E. coli |
Without catheter |
1 |
|
1 |
|
|
|
With catheter |
2.36 (1.28-4.34) |
0.006
|
1.86 (1-3.44) |
0.049
|
| E. coli source |
Non-urine |
1 |
|
1 |
|
|
|
Urine |
0.95 (0.52-1.73) |
0.87 |
0.52 (0.26-1.033) |
0.062 |
a Abbreviations: DM, Diabetes mellitus; HTN, Hypertension; IHD, ischemic heart diseases; CRF, chronic renal failure; BPH, benign prostatic hyperplasia; ISD, immunosuppressive drug; AB, antibiotic; UTI, urinary tract infection; ICU, intensive care unit; Uro, Uropathogenic; odds ratio; CI, confidence interval.
b All p values were calculated using binary logistic regression.
c other than FQ and SXT
Table 2.
laboratory factors associated with E. coli resistance to FQ and SXT as assessed by univariate analysisa
|
Risk Factors
|
Category
|
FQ OR (95% CI)
|
FQ
Pb value
|
SXT OR (95% CI)
|
SXT
Pb value
|
| WBC |
Normal |
1 |
|
1 |
|
|
|
Leukocytosis |
0.750 (0.45-1.24) |
0.26 |
0.95 (0.56-1.6) |
0.85 |
| Hb |
Normal |
1 |
|
1 |
|
|
|
Anemia |
2.16 (1.23-3.77) |
0.006
|
1.42 (0.79-2.55) |
0.25 |
| Plt |
Normal |
1 |
|
1 |
|
|
|
Thrombocytopenia |
0.74 (0.43-1.27) |
0.28 |
0.86 (0.49-1.52) |
0.61 |
| Creatinine |
Normal |
1 |
|
1 |
|
|
|
High |
1.15 (0.7-1.89) |
0.58 |
1.23 (0.74-2.06) |
0.43 |
| ESR |
Normal |
1 |
|
1 |
|
|
|
High |
1.42 (0.68-2.97) |
0.35 |
0.85 (0.38-1.9) |
0.69 |
| PCT |
Normal |
1 |
|
1 |
|
|
|
High |
1.11 (0.51-2.42) |
0.79 |
1.34 (0.57-3.16) |
0.51 |
a Abbreviations: WBC, white blood cell; Hb, Hemoglobin; Plt, platelet; ESR, Erythrocyte sedimentation rate; PCT, procalcitonin, OR, odds ratio; CI, confidence interval
b All p values were calculated using binary logistic regression.
Table 3.
Antibiogram- based factors associated with E. coli resistance to FQ and SXT as assessed by univariate analysisa
| Risk Factors |
Category
|
FQ OR (95% CI)
|
FQ P b value
|
SXT OR (95% CI)
|
SXT P b value
|
| ESBL |
No |
1 |
|
1 |
|
|
|
Yes |
9.01 (5.23-15.53) |
0.000
|
3.14 (1.88-5.26) |
0.000
|
| PTZ |
S |
1 |
|
1 |
|
|
|
R |
5.77 (0.73-45.37) |
0.069 |
1.57 (0.42-5.83) |
0.503 |
| CAR |
S |
1 |
|
- |
- |
|
|
R |
0.71 (0.65-0.77) |
0.559 |
- |
- |
| AN |
S |
1 |
|
1 |
|
|
|
R |
2.89 (0.63-13.32) |
0.17 |
6.38 (0.83-49.31) |
0.076 |
| GM |
S |
1 |
|
1 |
|
|
|
R |
11.69 (5.17-26.43) |
0.000
|
1.63 (0.94-2.83) |
0.083 |
| NIT |
S |
1 |
|
1 |
|
|
|
R |
2.48 (0.69-8.91) |
0.163 |
1.5 (0.47-4.78) |
0.49 |
| CTZ |
S |
1 |
|
1 |
|
|
|
R |
10.52 (5.96-18.56) |
0.000
|
3.12 (1.84-5.27) |
0.000
|
| CTX |
S |
1 |
|
1 |
|
|
|
R |
10.65 (5.99-18.93) |
0.000
|
3.34 (1.96-5.69) |
0.000
|
| CFZ |
S |
1 |
|
1 |
|
|
|
R |
8.38 (3.18-22.06) |
0.000
|
2.3 (0.92-5.78) |
0.076 |
| SXT |
S |
1 |
|
- |
|
|
|
R |
2.98 (1.77-5.03) |
0.000
|
- |
|
a Abbreviations: PTZ, piperacillin tazobactam; CAR, carbapenem; AN, amikacin; GM, gentamicin; NIT, nitrofurantoin; CTZ, ceftazidime; CTX, cefotaxime; CFZ, cefazolin; FQ, fluoroquinolone; SXT, cotrimoxazolee, OR,odds ratio; CI, confidence interval.
b All p values were calculated using binary logistic regression.
STX resistance
Regarding SXT, 70% of E. coli isolates were resistant. Univariate analysis demonstrated that prior antibiotic (other than FQ and SXT) use (P value = 0.002, OR = 2.3, 95% CI = 1.34-3.92), ICU admission (P value = 0.004, OR = 3.23, 95% CI = 1.41-7.48), urinary catheterization (P value = 0.049, OR = 1.86, 95% CI = 1-3.44) (Table 1), ESBL production (P value = 0.000, OR = 3.14, 95% CI = 1.88-5.26), FQ resistance (P value = 0.000, OR = 2.98, 95% CI = 1.77-5.03) were found to be statistically significant risk factors for SXT resistance. There was a trend toward significance for the male sex (P value = 0.081, OR = 1.57, 95% CI = 0.946-2.607), prior FQ (P value = 0.065, OR = 1.84, 95% CI = 0.96-3.53) (Table 1), gentamicin (P value = 0.083, OR = 1.63, 95% CI = 0.94-2.83), and AN administration (P value = 0.076, OR = 6.38, 95% CI = 0.83-49.31) (Table 3).
Furthermore, multivariate analysis of independent risk factors for E. coli resistance to FQs and SXT are displayed in Table 4. Our findings showed that type II diabetes mellitus, prior urinary tract infection, gentamicin resistance, prior FQ use, and ESBL were statistically significant risk factors for E. coli resistance to FQs and SXT.
Table 4.
Multivariate analysis of independent risk factors for E. coli resistance to FQs and SXT a
|
Risk Factors
|
Category
|
OR (95% CI)
|
Pb value
|
|
For FQ
|
|
|
|
| DM |
No |
1 |
|
|
|
Yes |
2.24 (1.05-4.8) |
0.038 |
| Prior UTI |
No |
1 |
|
|
|
Yes |
5.92 (1.25-28.1) |
0.025 |
| GM |
S |
1 |
|
|
|
R |
11.68 (3.63-37.6) |
0.000 |
| Prior FQ use |
No |
1 |
|
|
|
Yes |
3.1 (0.86-10.65) |
0.049 |
| ESBL |
No |
1 |
|
|
|
Yes |
9.43 (4.32-20.59) |
0.000 |
|
For SXT
|
|
|
|
| ESBL |
No |
1 |
|
|
|
Yes |
3 (1.62-5.57) |
0.000 |
a Abbreviations. OR, odds ratio; CI, confidence interval
b All p values were calculated using logistic regression.
Discussion
The prevalence of antibiotic resistance, resistance patterns, and associated risk factors may vary among different geographic locations. This study investigated the prevalence of FQs and STX-resistant E. coli and the related risk factors in the Northwest of Iran. The present study investigated E. coli isolates from community-acquired and nosocomial infections obtained from urine, blood, respiratory secretion, and wound.
In the United States, Fluit et al reported that the resistance rate of E. coli to FQ was 4.7-7.9% in 200014; however, there was no resistance to FQ among E. coli isolates in 1997.28 In 2008, Talan et al indicated that the prevalence of FQ and SXT-resistant E. coli was 5% and 24% among patients with pyelonephritis in the United States.15 In the United States, the rate of resistance to SXT increased from 15.4% to 25.1% from 1997 to 2018,14,15,28 and the resistance for FQ increased from < 1% to approximately 30% from 1997 to 2015.14,15,28,29 In India, the prevalence rate of FQ and SXT was 89% and 94% among patients with gastrointestinal infections.13 It has been reported that antimicrobial resistance in community-acquired uropathogenic E. coli isolates to FQ and SXT was 17.8% and 34.2%, respectively.6 In Iran, the rate of E. coli resistance to SXT and FQ was 64% and 28%,11 which was approximately retained at 62% in 2019.16 In our study, the prevalence rate of E. coli resistance to FQ and SXT was 66.3% and 70%, respectively. The widespread use of SXT and the increasing E. coli resistance to this antibiotic encouraged clinicians to use FQs as suitable alternatives for most infections because of their high potency, broad spectrum, and tolerability. Our results have demonstrated worrisome emergence of E. coli resistant to FQs.
The present study also investigated the potential risk factors for developing FQs and STX-resistant E. coli in the Northwest of Iran. The current study is among the few studies investigating the relationship of underlying diseases with E. coli resistance to FQ and SXT. Our results have indicated that among nephrolithiasis, diabetes mellitus, hypertension, ischemic heart diseases, chronic renal failure, and cancer, only type II diabetes mellitus is a risk factor for FQ-resistant E. coli. In line with the previous findings,1,23 our results have shown that prior urinary tract infections and urinary catheterization are risk factors for FQ-resistant E. coli. Consistent with previous reports,1,3,4 our results have indicated that the resistance to FQ and SXT is related to the recent administration of FQ and other antibiotics. Consistent with the study by Sotto et al,30 our findings have indicated that ICU admission was associated with SXT resistance but not with FQ. In addition, the administration of immunosuppressive drugs and smoking, similar to earlier findings, were not associated with FQ or SXT resistance4; however, Zhu et al reported that immunosuppressive drugs were risk factors for FQ resistance.1 Our study has demonstrated that 74%-81% of ESBL-producing E. coli were significantly resistant to FQ and SXT; these results were compatible with the previous studies.9,14,24 Furthermore, our findings have indicated that resistance to gentamicin and SXT is associated with FQ resistance, and resistance to FQ is associated with resistance to SXT. However, our results have shown that sex and age are the risk factors for developing STX-resistant E. coli, probably due to their excessive use in all age groups in our region. In accordance with our findings, it has been reported that sex and age were not related to FQ or SXT resistance.13 In contrast, earlier studies demonstrated that male sex and age above 65 were independent risk factors for resistance to FQ or SXT.1,3,4,6 To the best of our knowledge, the current study is among the studies that investigated the association of the laboratory parameters, including leukocytosis, anemia, thrombocytopenia, creatinine, erythrocyte sedimentation rate, and procalcitonin levels, with FQ and SXT-resistant E. coli. Our results have demonstrated that only anemia is associated with FQ and SXT-resistant E. coli. However, due to the possibility of having different risk factors for colonization and infection, it is recommended that these two groups be separately investigated further in future studies.
Conclusion
With a prevalence rate above 65%, FQ and SXT-resistant E. coli infectionshave become an emerging concern in our region. Based on multivariant analyses, type II diabetes mellitus, prior urinary tract infection, gentamicin resistance, prior FQ administration, and ESBL production are risk factors for developing FQ-resistant E. coli and ESBL production is the risk factor for developing STX-resistant E. coli in our region.
Competing Interests
The authors have no conflicts of interest to declare.
Ethical Approval
This study was approved by the Ethics Committee of Tabriz University of Medical Sciences, Tabriz, Iran (IR.TBZMED.REC.1400.084) and the informed consent was obtained from the patients.
Acknowledgements
The authors would like to thank the Infectious and Tropical Diseases Research Center, Tabriz University of Medical Sciences, Tabriz, Iran and Clinical Research Development Unit of Sina Educational, Research and Treatment Center, Tabriz University of Medical Sciences, Tabriz, Iran for their assistance.
References
- Zhu DM, Li QH, Shen Y, Zhang Q. Risk factors for quinolone-resistant Escherichia coli infection: a systematic review and meta-analysis. Antimicrob Resist Infect Control 2020; 9(1):11. doi: 10.1186/s13756-019-0675-3 [Crossref] [ Google Scholar]
- Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases E-Book. Elsevier Health Sciences; 2019.
- Lautenbach E, Fishman NO, Bilker WB, Castiglioni A, Metlay JP, Edelstein PH. Risk factors for fluoroquinolone resistance in nosocomial Escherichia coli and Klebsiella pneumoniae infections. Arch Intern Med 2002; 162(21):2469-77. doi: 10.1001/archinte.162.21.2469 [Crossref] [ Google Scholar]
- Rattanaumpawan P, Tolomeo P, Bilker WB, Fishman NO, Lautenbach E. Risk factors for fluoroquinolone resistance in gram-negative bacilli causing healthcare-acquired urinary tract infections. J Hosp Infect 2010; 76(4):324-7. doi: 10.1016/j.jhin.2010.05.023 [Crossref] [ Google Scholar]
- Muratani T, Matsumoto T. Urinary tract infection caused by fluoroquinolone- and cephem-resistant Enterobacteriaceae. Int J Antimicrob Agents 2006; 28 Suppl 1:S10-3. doi: 10.1016/j.ijantimicag.2006.05.009 [Crossref] [ Google Scholar]
- Rocha JL, Tuon FF, Johnson JR. Sex, drugs, bugs, and age: rational selection of empirical therapy for outpatient urinary tract infection in an era of extensive antimicrobial resistance. Braz J Infect Dis 2012; 16(2):115-21. doi: 10.1016/s1413-8670(12)70291-x [Crossref] [ Google Scholar]
- Karaca Y, Coplu N, Gozalan A, Oncul O, Citil BE, Esen B. Co-trimoxazole and quinolone resistance in Escherichia coli isolated from urinary tract infections over the last 10 years. Int J Antimicrob Agents 2005; 26(1):75-7. doi: 10.1016/j.ijantimicag.2005.03.012 [Crossref] [ Google Scholar]
- Ishihara S, Yokoi S, Masue N, Yamada T, Minamidate Y, Yasuda M. Urinary tract-derived Escherichia coli resistant to co-trimoxazole in Japan, where the drug is seldom used for treating acute urinary tract infections. J Antimicrob Chemother 2002; 49(5):881-2. doi: 10.1093/jac/dkf015 [Crossref] [ Google Scholar]
- Marwa KJ, Mushi MF, Konje E, Alele PE, Kidola J, Mirambo MM. Resistance to cotrimoxazole and other antimicrobials among isolates from HIV/AIDS and Non-HIV/AIDS patients at Bugando Medical Centre, Mwanza, Tanzania. AIDS Res Treat 2015; 2015:103874. doi: 10.1155/2015/103874 [Crossref] [ Google Scholar]
- Wang Q, Zhao K, Guo C, Li H, Huang T, Ji J. Antibiotic resistance and virulence genes of Escherichia coli isolated from patients with urinary tract infections after kidney transplantation from deceased donors. Infect Drug Resist 2021; 14:4039-46. doi: 10.2147/idr.S332897 [Crossref] [ Google Scholar]
- Rezaei-Tavirani M, Ghafourian S, Sayehmiri F, Pakzad R, Safiri S, Pakzad I. Prevalence of cotrimoxazole resistance uropathogenic bacteria in Iran: a systematic review and meta-analysis. Arch Clin Infect Dis 2018; 13(5):e63256. doi: 10.5812/archcid.63256 [Crossref] [ Google Scholar]
- Zhanel GG, Karlowsky JA, Harding GK, Carrie A, Mazzulli T, Low DE. A Canadian national surveillance study of urinary tract isolates from outpatients: comparison of the activities of trimethoprim-sulfamethoxazole, ampicillin, mecillinam, nitrofurantoin, and ciprofloxacin The Canadian Urinary Isolate Study Group. Antimicrob Agents Chemother 2000; 44(4):1089-92. doi: 10.1128/aac.44.4.1089-1092.2000 [Crossref] [ Google Scholar]
- Rath S, Padhy RN. Prevalence of fluoroquinolone resistance in Escherichia coli in an Indian teaching hospital and adjoining communities. J Taibah Univ Med Sci 2015; 10(4):504-8. doi: 10.1016/j.jtumed.2015.02.009 [Crossref] [ Google Scholar]
- Fluit AC, Jones ME, Schmitz FJ, Acar J, Gupta R, Verhoef J. Antimicrobial susceptibility and frequency of occurrence of clinical blood isolates in Europe from the SENTRY antimicrobial surveillance program, 1997 and 1998. Clin Infect Dis 2000; 30(3):454-60. doi: 10.1086/313710 [Crossref] [ Google Scholar]
- Talan DA, Krishnadasan A, Abrahamian FM, Stamm WE, Moran GJ. Prevalence and risk factor analysis of trimethoprim-sulfamethoxazole- and fluoroquinolone-resistant Escherichia coli infection among emergency department patients with pyelonephritis. Clin Infect Dis 2008; 47(9):1150-8. doi: 10.1086/592250 [Crossref] [ Google Scholar]
- Noie Oskouie A, Hasani A, Ahangarzadeh Rezaee M, Soroush Bar Haghi MH, Hasani A, Soltani E. A relationship between O-serotype, antibiotic susceptibility and biofilm formation in uropathogenic Escherichia coli. Microb Drug Resist 2019; 25(6):951-8. doi: 10.1089/mdr.2018.0330 [Crossref] [ Google Scholar]
- Kern WV, Andriof E, Oethinger M, Kern P, Hacker J, Marre R. Emergence of fluoroquinolone-resistant Escherichia coli at a cancer center. Antimicrob Agents Chemother 1994; 38(4):681-7. doi: 10.1128/aac.38.4.681 [Crossref] [ Google Scholar]
- Colgan R, Johnson JR, Kuskowski M, Gupta K. Risk factors for trimethoprim-sulfamethoxazole resistance in patients with acute uncomplicated cystitis. Antimicrob Agents Chemother 2008; 52(3):846-51. doi: 10.1128/aac.01200-07 [Crossref] [ Google Scholar]
- Sannes MR, Belongia EA, Kieke B, Smith K, Kieke A, Vandermause M. Predictors of antimicrobial-resistant Escherichia coli in the feces of vegetarians and newly hospitalized adults in Minnesota and Wisconsin. J Infect Dis 2008; 197(3):430-4. doi: 10.1086/525530 [Crossref] [ Google Scholar]
- Bailey AM, Weant KA, Baker SN. Prevalence and risk factor analysis of resistant Escherichia coli urinary tract infections in the emergency department. Pharm Pract (Granada) 2013; 11(2):96-101. doi: 10.4321/s1886-36552013000200006 [Crossref] [ Google Scholar]
- Ena J, Amador C, Martinez C, Ortiz de la Tabla V. Risk factors for acquisition of urinary tract infections caused by ciprofloxacin resistant Escherichia coli. J Urol 1995; 153(1):117-20. doi: 10.1097/00005392-199501000-00040 [Crossref] [ Google Scholar]
- Abdu A, Kachallah M, Bolus DY. Antibiotic susceptibility patterns of uropathogenic Escherichia coli among patients with urinary tract infections in a tertiary care hospital in Maiduguri, north-eastern Nigeria. J Biosci Biotechnol Discov 2018; 3:14-24. [ Google Scholar]
- Gangcuangco LM, Alejandria M, Henson KE, Alfaraz L, Ata RM, Lopez M. Prevalence and risk factors for trimethoprim-sulfamethoxazole-resistant Escherichia coli among women with acute uncomplicated urinary tract infection in a developing country. Int J Infect Dis 2015; 34:55-60. doi: 10.1016/j.ijid.2015.02.022 [Crossref] [ Google Scholar]
- Lautenbach E, Strom BL, Bilker WB, Patel JB, Edelstein PH, Fishman NO. Epidemiological investigation of fluoroquinolone resistance in infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Clin Infect Dis 2001; 33(8):1288-94. doi: 10.1086/322667 [Crossref] [ Google Scholar]
- Chan YQ, Chen K, Chua GT, Wu P, Tung KT, Tsang HW. Risk factors for carriage of antimicrobial-resistant bacteria in community dwelling-children in the Asia-Pacific region: a systematic review and meta-analysis. JAC Antimicrob Resist 2022; 4(2):dlac036. doi: 10.1093/jacamr/dlac036 [Crossref] [ Google Scholar]
- Tille PM. Bailey & Scott’s Diagnostic Microbiology-E-Book. Elsevier Health Sciences; 2021.
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing: 20th Informational Supplement. CLSI Document M100-S20. Wayne, PA: CLSI; 2021.
- Chomarat M. Resistance of bacteria in urinary tract infections. Int J Antimicrob Agents 2000; 16(4):483-7. doi: 10.1016/s0924-8579(00)00281-8 [Crossref] [ Google Scholar]
- Spellberg B, Doi Y. The rise of fluoroquinolone-resistant Escherichia coli in the community: scarier than we thought. J Infect Dis 2015; 212(12):1853-5. doi: 10.1093/infdis/jiv279 [Crossref] [ Google Scholar]
- Sotto A, De Boever CM, Fabbro-Peray P, Gouby A, Sirot D, Jourdan J. Risk factors for antibiotic-resistant Escherichia coli isolated from hospitalized patients with urinary tract infections: a prospective study. J Clin Microbiol 2001; 39(2):438-44. doi: 10.1128/jcm.39.2.438-444.2001 [Crossref] [ Google Scholar]