J Res Clin Med. 13:34784.
doi: 10.34172/jrcm.025.34784
Original Article
Role of ultrasound scan and fine needle aspiration cytology on pre-operative assessment of suspicious thyroid nodules in a resource-limited setting
Kulatunga Mudiyanselage Hiroshani Hansamali Kulatunga Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing, 1 
Ajith Aloka Pathirana Conceptualization, Methodology, Resources, Supervision, Validation, Writing – review & editing, 2
Sarrikkalige Suhasini Neluka Fernando Conceptualization, Funding acquisition, Supervision, Validation, Writing – review & editing, 3
Bawantha Dilshan Gamage Conceptualization, Methodology, Resources, Supervision, Writing – review & editing, 2
Magala Kottahachchige Asanga Sampath Conceptualization, Supervision, Writing – review & editing, 4
Cherine Sosai Resources, Validation, Writing – review & editing, 5
Surangi Jayakody Formal analysis, Resources, Writing – review & editing, 6
Bimalka Samanthi Seneviratne Conceptualization, Funding acquisition, Methodology, Resources, Validation, Writing – review & editing, 1, *
Author information:
1Department of Pathology, Faculty of Medical Sciences, University of Sri Jayewardenepura, Nugegoda, Sri Lanka
2Department of Surgery, Faculty of Medical Sciences, University of Sri Jayewardenepura, Nugegoda, Sri Lanka
3Department of Microbiology, Faculty of Medical Sciences, University of Sri Jayewardenepura, Nugegoda, Sri Lanka
4Department of Basic Sciences, Faculty of Allied Health Sciences, University of Sri Jayewardenepura, Nugegoda, Sri Lanka
5Department of Pathology, Colombo South Teaching Hospital, Colombo, Sri Lanka
6Department of Community Medicine, Faculty of Medical Sciences, University of Sri Jayewardenepura, Nugegoda, Sri Lanka
Abstract
Introduction:
Although the prevalence of thyroid tumor is about 7% in the general population, the malignancy rate is approximately 5% among thyroid tumors. This emphasizes the need for effective preoperative diagnostic methods for proper patient management.
Methods:
A descriptive cross-sectional study was conducted at Colombo South Teaching Hospital and the Department of Pathology, University of Sri Jayewardenepura, Sri Lanka. Patients with radiologically suspected malignant thyroid nodules (n=107) were enrolled. fine needle aspiration cytology (FNAC) was performed under ultrasound scan (USS) guidance by an experienced consultant radiologist. Direct smears and cell block preparations were prepared from FNAC specimens. Smears were reviewed by two independent pathologists. USS and FNAC findings were reported according to Thyroid Imaging Reporting and Data System (TIRADS) system and Bethesda system, respectively. Descriptive statistics were expressed as frequencies and percentages. Diagnostic performance of USS and FNAC was assessed using receiver operating characteristic (ROC) curve. Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) were calculated.
Results:
The Majority (79.4%) were females. Age ranged from 15 to 76 years (47.3±12.89). Malignant risk prediction of 77% was observed in TIRADS system. Malignant risk of 17.9%, 37.5%, and 87.5% were reported respectively for TIRADS 4a, 4b, 4c categories while TIRADS 5 reports a risk of 60.0%. Sensitivity, specificity, NPV, and PPV of FNAC were 88.9%, 87.5%, 96%, and 70% respectively compared with the histology results.
Conclusion:
Bethesda system cytology reporting and radiologic TIRADS classification are important preoperative diagnostic tools for identifying suspicious thyroid nodules in resource-limited setting. FNAC was a better diagnostic test compared to USS for evaluating thyroid nodules.
Keywords: Fine needle aspiration, Thyroid malignancy, Ultrasound scan
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This study was supported by the Cancer Research Grant (Grant No. 002/2019) and the University Research Grant (ASP/MED/01/2021/55) from the University of Sri Jayewardenepura, Sri Lanka.
Introduction
Thyroid tumours are more prevalent than tumours arising from other organs of the endocrine system. The incidence of thyroid carcinoma has tripled in the United States and other countries over the past three decades, and this trend shows no signs of abating.1 A global prevalence of 24.83% has been reported for thyroid nodules from 2012 to 2022, with women (36.51%) more affected than men (24.47%).2 In Sri Lanka, there is a 2.1-fold increase in the incidence of thyroid carcinoma from 2001 to 2010.3 Recent cancer incidence data from Sri Lanka emphasize the gravity of the situation. According to the latest cancer incidence data (2021), thyroid cancer is reported as the second most common type of malignancy in females in Sri Lanka. However, despite a relatively high prevalence of thyroid tumors (7% of the population), only about 5% are malignant.4
In lower-middle-income countries like Sri Lanka, limited healthcare resources make the rising burden of thyroid cancer particularly challenging. Furthermore, the costs associated with surgical management are notably high. The current lack of operating theater capacity also restricts the surgical management of thyroid nodules. Therefore, the decision of surgical management is taken based on the clinical features and the diagnostic test results. Given the increasing incidence of thyroid carcinoma, effective methods are essential because prognosis and treatment depend on the type and stage of the nodule.5 However, there are reported cases of re-operations and unwanted surgeries due to mistakes in pre-operative diagnosis.
Ultrasound scan (USS) of the thyroid and the fine needle aspiration cytology (FNAC) are widely used preoperative diagnostic methods. Thyroid Imaging Reporting and Data System (TIRADS) which was proposed in 2015 by the American College of Radiologists is currently in practice to standardize the interpretations of the thyroid ultrasound scan results. This system uses a standardized scoring system based on composition, echogenicity, shape, margin, and echogenic foci. The TIRADS system categorizes nodules into five groups from TIRADS 1 to TIRADS 5 based on a standardized score.6
Another well-established pre-operative diagnostic approach is the FNAC. This technique can be performed with or without ultrasound guidance. This investigation plays a major role in the pre-operative diagnosis as it is used to stratify the patients with a risk of malignancy, therefore enabling the identification of patients requiring surgery thus preventing unnecessary surgeries for benign nodules. Thyroid nodules are classified into six categories according to the Bethesda system for reporting thyroid cytopathology. Overall, 20-30% of nodules fall into Bethesda categories III, IV, and V, which are considered indeterminate or suspicious. However, prior reports indicate that malignancy is confirmed histologically in only about one-third of these indeterminate nodules.6,7
Histopathological diagnosis is considered the gold standard in the diagnosis of thyroid malignancies. Although it is the gold standard, obtaining tissue requires hemithyroidectomy or total thyroidectomy.
Although currently, in the Sri Lankan context, there is access to a variety of pre-operative diagnostic methodologies, it is crucial to evaluate the diagnostic accuracy of these methods due to their significant influence on the disease prognosis. This will help to prevent unwanted surgical procedures and subsequent re-operations on thyroid nodules. The purpose of the current study is to determine the diagnostic accuracy of the TIRADS system of USS and Bethesda system of FNAC in the preoperative diagnosis of thyroid tumors.
Methods
A descriptive cross-sectional study was conducted at the Department of Radiology, Colombo South Teaching Hospital, and the Department of Pathology, Faculty of Medical Sciences (FMS) of the University of Sri Jayewardenepura, Sri Lanka from June 2020 to June 2022 enrolling 107 patients with radiologically suspicious thyroid nodules (TIRADS 3 or above). All procedures were approved by the Ethics Review Committee of the Faculty of Medical Sciences of the University of Sri Jayewardenepura (65/2019) and approval was granted to conduct the study. Written informed consent was obtained from each participant. Cases without radiological data and patients belonging to TIRADS 1 and 2 categories (as there were no indications for FNAC) were excluded from the study.
All ultrasound scans were performed by the same consultant radiologist and reported using the five categories.3 Ultrasound-guided FNAC was performed by the same radiologist when nodules were suspicious for malignancy. Direct smears were prepared and fixed in 95% ethanol for routine hematoxylin and eosin staining. Residual material in the needle was rinsed into an ethanol formalin solution. The needle wash sample was used for the cell block preparation. Both direct cytology smears and cell-block sections were reviewed by two independent pathologists and reported according to the Bethesda system. Inter-observer variation was minimized by having the same radiologist perform and report all USS examinations according to TIRADS. Further, the same radiologist collected the FNAC samples from the suspected nodule, and cytology smears were observed by two independent pathologists adhering to the Bethesda system. If discrepancies arose, both consultant pathologists discussed and decided on the final diagnosis.
The patients were followed up for two years, and the histology reports were collected from the patients if they underwent surgery. Patients with benign nodules did not undergo surgery hence there were no histological reports. Patients who did not undergone surgery were followed by the research team for two years from the date of FNAC. If the nodules did not develop further or if they had been confirmed as benign nodules by a consultant surgeon or an endocrinologist, the nodule was considered benign at the end of the follow-up period.
The results were analyzed using the SPSS statistical software version 23. Descriptive statistics were expressed in terms of frequencies and percentages. The receiver operator characteristic (ROC) curve was used to assess the diagnostic performance of USS and FNAC. Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) were calculated. Kendall’s coefficient of concordance was used to compare the concordance rates of USS and FNAC with the final histology results. A P value of < 0.05 was considered statistically significant.
Results
From the total of one hundred and seven (n = 107) participants, the majority (n = 85, 79.4%) were female. The age of the study participants ranged from 15 to 76 years of age with a mean and standard deviation (SD) of 47.3 ± 12.89 years.
All the nodules were TIRADS 3 or above, as only radiologically suspicious thyroid nodules were included in the study. Radiology revealed that 20.6% (n = 22) were TIRADS 3 (mildly suspicious), 74.8% (n = 80) TIRADS 4 (moderately suspicious), and 4.7% (n = 5) TIRADS 5 (highly suspicious), respectively. Within TIRADS 4, 52.3% (n = 56) were 4a, 7.5% (n = 8) were 4b, and 15% (n = 16) were 4c, based on the level of suspiciousness (Table 1).
Table 1.
Baseline characteristics of radiological and cytological features
|
Radiology results – According to TIRADS classification (n=107)
|
Cytological results – According to the Bethesda system (n=107)
|
|
TIRADS category
|
Frequency
|
Bethesda category
|
Frequency
|
| TIRADS 3 |
22 |
Bethesda 1 |
14 |
| TIRADS 4a |
56 |
Bethesda 2 |
44 |
| TIRADS 4b |
08 |
Bethesda 3 |
15 |
| TIRADS 4c |
16 |
Bethesda 4 |
06 |
| TIRADS 5 |
05 |
Bethesda 5 |
20 |
|
|
|
Bethesda 6 |
08 |
Cytology results were reported according to the Bethesda system. Among the 107 participants, the majority (n = 43, 40.2%) were in the Bethesda 2 category followed by Bethesda 5, 3, 1, 6, and 4 as shown in Table 1.
When the TIRADS system (radiological) results were compared with the cytology results of the study sample, of the 22 mildly suspicious (TIRADS 3) nodules, the majority were classified as benign according to cytological features (n = 20). Only 2 of these TIRADS 3 nodules were reported as Bethesda 5 (suspicious of malignancy) or Bethesda 6 (malignant). In the TIRADS 4a category, the majority were benign (n = 48). Only 7 nodules in the TIRADS 4a category were Bethesda 5, and 1 was reported in Bethesda 6 category. In TIRADS 4b, the majority (n = 6) were cytologically benign (Bethesda 1, 2, 3 and 4) while one nodule each was Bethesda 5 and Bethesda 6 (malignant). However, in the TIRADS 4c, the majority (n = 14) were reported as malignant and included 9 nodules in Bethesda 5 and another 5 in Bethesda 6. In the TIRADS 5 category, 3 nodules out of 5 were cytologically benign while the remaining 2 were malignant (n = 1 in Bethesda 5 and n = 1 in Bethesda 6).
Of the 44 available histology reports, 29 were papillary thyroid carcinoma (Papillary thyroid carcinoma n = 24, Cystic papillary carcinoma n = 1, Papillary microcarcinoma n = 2, Follicular variant of papillary thyroid carcinoma n = 2), while 13 were benign thyroid nodules (TIRADS 3 = 3, TIRADS 4a = 10). Further, all nodules in TIRADS 4b, 4c and 5 were histologically papillary thyroid carcinomas.
The malignancy risk of each TIRADS category was seen to significantly rise with the increase in the TIRADS categories except for category 5. With the follow-up of 107 patients, the TIRADS 4a, 4b, and 4c categories had a malignant risk of 13.6%, 17.9%, 37.5%, and 87.5%, respectively, while TIRADS 5 reported a risk of 60.0% (Table 2).
Table 2.
Proportion of malignancy risk in each TIRADS category
|
TIRADS category
|
Follow up
|
Total
|
Proportion of malignant risk
|
|
Benign
|
Malignant
|
| TIRADS 3 |
19 |
3 |
22 |
13.6% |
| TIRADS 4a |
46 |
10 |
56 |
17.9% |
| TIRADS 4b |
5 |
3 |
8 |
37.5% |
| TIRADS 4c |
2 |
14 |
16 |
87.5% |
| TIRADS 5 |
2 |
3 |
5 |
60.0% |
From the enrolled 107 radiologically malignancy-suspicious thyroid nodules, only 28 (26.16%) were diagnosed as suspicious of malignancy (Bethesda 5) or malignant (Bethesda 6) according to the FNAC findings. The majority of the nodules (n = 43, 40.2%) belonged to Bethesda 2 category, which is considered benign. Total or hemi-thyroidectomies was performed in all 28 cytologically malignancy-suspected patients. Of these, 92.8%, (n = 26) were confirmed malignant following histological assessment. Two patients with cytologically malignant nodules were diagnosed with benign papillary hyperplasia and multinodular goiter with thyroiditis following histological follow-up.
The proportion of malignancy risk rose with increasing Bethesda category compared with the histopathological data. Malignancy risk of 95% and 100% were reported in Bethesda 5 and 6,which are considered suspicious for malignancy and malignant, respectively (Table 3).
Table 3.
Proportion of malignancy risk of each Bethesda category
|
Bethesda category
|
Follow-up
|
Total
|
Percentage risk
|
|
Benign count
|
Malignant count
|
| Bethesda 1 |
13 |
1 |
14 |
7.1% |
| Bethesda 2 |
41 |
2 |
43 |
4.7% |
| Bethesda 3 |
15 |
1 |
16 |
6.3% |
| Bethesda 4 |
4 |
2 |
6 |
33.3% |
| Bethesda 5 |
1 |
19 |
20 |
95.0% |
| Bethesda 6 |
0 |
8 |
8 |
100% |
Sensitivity, specificity, negative predictive value and the positive predictive value of the FNAC technique were found to be 88.9%, 87.5%, 96% and 70% respectively, while those of the TIRADS classification were 89.04%, 30.30%, 55.56% and 73.86% respectively, when compared with e histology results.
Further, cell blocks were also prepared from the same cytology specimens and a highly statistically significant association was observed between the cell block cytology and direct FNAC according to Fisher’s exact test (P = 0.000).
A statistically significant association was observed between the Bethesda system and final histology results (P < 0.05) according to the Fisher’s Exact test. Also, perfect agreement (84.0%) was observed between the Bethesda system of reporting FNAC and histology result according to the kappa statistics.
Statistically significant positive correlation was observed between the TIRADS system of USS and Bethesda system of reporting thyroid cytology results (r = 0.35, P < 0.05). Higher TIRADS and Bethesda categories were associated with malignancies according to histological results.
When USS TIRADS and FNAC were compared as tools of pre-operative diagnosis using the ROC curve, the Bethesda system had a larger area under the curve (0.73) than USS TIRADS (0.65). Hence, FNAC was a better diagnostic test than USS in the evaluation of thyroid nodules (Figure 1).
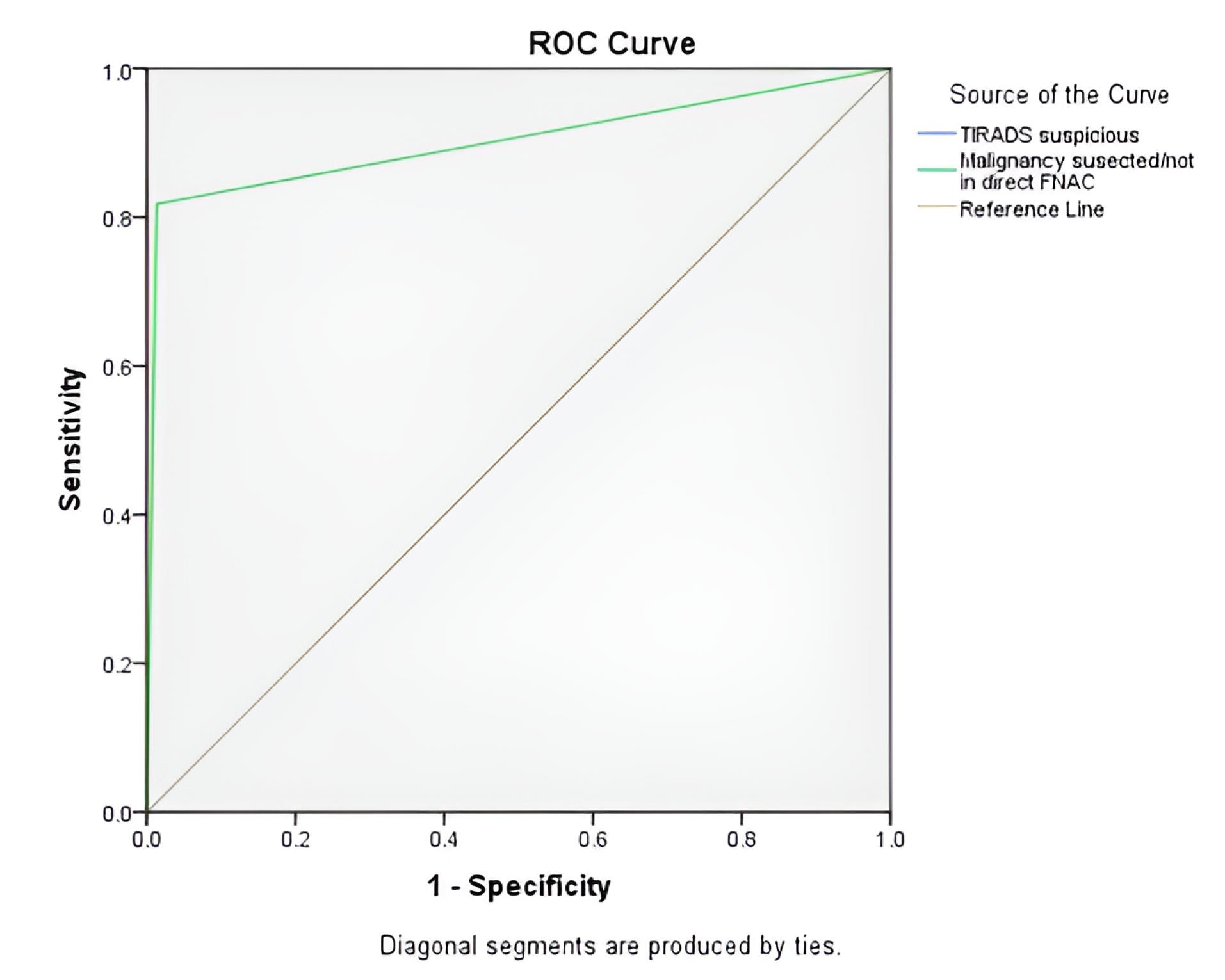
Figure 1.
ROC curve for the TIRADS classification and Bethesda Classification. AUC=0.5: Model performs like random guessing., AUC=1.0: Model perfectly separates positive and negative cases, AUC>0.5: Model has some ability to predict correctly
.
ROC curve for the TIRADS classification and Bethesda Classification. AUC=0.5: Model performs like random guessing., AUC=1.0: Model perfectly separates positive and negative cases, AUC>0.5: Model has some ability to predict correctly
Overall concordance of 68.6% was reported among USS TIRADS, the Bethesda system of FNAC and final histology results according to Kendall’s coefficient of concordance.
Discussion
According to the findings of the current study, thyroid tumors are common in females of middle age. This is in line with most of other published literature which reports thyroid tumors ranging from 61% to 93% with a female preponderance.7-9 Although a specific reason cannot be found for this preponderance, it may be due to the X-chromosome inactivation as seen in the etiology of autoimmune thyroiditis and hormonal effects.10 Though there is a female preponderance, according to a cancer incidence report from China, Korea and Japan, an upward trend in thyroid carcinoma incidence among males has been reported.11
Majority of radiologically suspicious nodules in TIRADS 4c were histologically proven to be malignant. Further, those nodules in TIRADS 4c showed a positive correlation with Bethesda categories 5 and 6. This finding of TIRADS 4c radiologically is an important factor to predict the risk of malignancy preoperatively and thus help in surgical management. In keeping with the findings of this study, George et al reported that there is a significantly high malignant risk in TIRADS 4 and 5 nodules compared to lower categories.12 The reported malignancy risk of 87.5% in 4c category of the current study is comparable to the reported 85% as seen in the study by Fernández Sánchez and 83.33% in De et al.13,14 Further, Kwak et al also reported that there is a malignant probability of 50-95% in the nodules of TIRADS 4c.15 Thus, the findings of the current study highlight the significance of TIRADS 4c category in pre-operative diagnosis of suspicious thyroid nodules in a resource-poor setting.
Further, present study also reported a large number of malignant thyroid nodules categorized as TIRADS 4c in this study setting. This may be due to the overlap of radiological findings between TIRADS 4c and TIRADS 5 category. As documented by Fernández Sánchez in 2014, TIRADS 4c and 5 category have overlapping features thus making it difficult to separate the two categories.13
Malignancy risk of 13.6%, 17.9%, 37.5%, 87.5% and 60% were reported respectively for the TIRADS 3, 4a, 4b, 4c, and 5 categories in the current study. Keeping in line with the current study, Srinivas reports a malignant risk of 0.64%, 4.76%, 66.67%, 83.33% and 100% respectively for TIRADS 3, 4a, 4b, 4c and 5.16 Another Indian study reports a malignant risk of 2.2%, 38.5%, and 77.8%, respectively for the TIRADS 3, TIRADS 4 and TIRADS 5 categories.17 A slight deviation in the malignant risk for TIRADS 5 category was observed in the current study, compared with other reported studies. Reduced number of specimens in TIRADS 5 category and overlapping of the features in 4c and 5 categories may be the main reason for this deviation.
Only 93% of the patients cytologically suspected of malignancy were histologically confirmed malignant, with a false-positive rate of 7%. False positive results were observed in two cases of multinodular goiter with thyroiditis in the current study. In keeping with this study, Krišto et al reported 3% false positive rate8 and 1.2% false positive rate of FNAC in Nandedkar et al.18 The main reasons for the cyto-histologic disagreement of some nodules are due to the overdiagnosis of thyroid nodules, due to autoimmune thyroiditis and papillary hyperplasia.19
A rise in the malignancy risk proportion was observed with the increase of the Bethesda system category (33.3%, 95.0% and 100% respectively, for Bethesda 4, 5, and 6 respectively) in the current study. Similar findings have been reported in Jo et al, giving malignancy risk proportions of 15-30% in Bethesda 4 and 97-99% in category 6.20 However, near 100% risks were observed in the Bethesda 5 category in many published reports, which are in line with the current study.9,21 These findings emphasize the diagnostic reliability of the Bethesda system of thyroid FNAC. In the current study, papillary thyroid carcinoma was diagnosed as the most common type of malignancy, accounting for 77.4% (24/31) of the available histology results. Papillary thyroid carcinoma incidence varied from 79.5% to 95%.22-24 However, the high prevalence of papillary thyroid carcinoma observed may be due to advancements in histological diagnostic criteria and the increased diagnostic ability of tumors.
TIRADS system had higher sensitivity (89.4%) and lower specificity (30.30%) to detect malignancy in the present study population. These sensitivity and specificity results are in line with De et al,14 Chaigneau et al,25 and Horvath et al,6 who reported sensitivity values ranging from 80%-92% and specificity ranging from 15-49% respectively. The present study findings revealed a higher positive predictive value (73.86%) and a lower negative predictive value (55.56%). Although the findings of Chaigneau et al, 25 (PPV = 79.5%, and NPV = 58.8%) are comparable with the current study, De et al14 (PPV = 51.28%, and NPV = 77.27%), and Horvath et al6 (PPV = 49.0%, and NPV = 88.0%), reported controversial results of higher NPV and lower PPV. However, Horvath et al6 reported a comparatively higher accuracy (94%) than the reported accuracy of 70.75% of the present study while De et al14 and Chaigneau et al25 reported 61% and 42.5% accuracy values respectively. Although a standard guideline is followed for reporting ultrasound scan findings, inter-observer variations may have been reasons for the observed variations. Similar to Dy et al, the current study findings also revealed that TIRADS classification is a sensitive classification system to identify malignant cases.26 Therefore, TIRADS classification can be utilized for the identification of malignant nodules during the pre-operative period.
The current study showed a sensitivity of 81.8% and specificity of 98.6% for detection of thyroid malignancy by the Bethesda system in FNAC. Similarly, George et al12 found a 78.72% sensitivity, 100% specificity in a study done in Kerala, India which included a study population of 150. Many other studies have reported comparable sensitivities (81.5% in Al-Dabbagh A, Ibraheem,7 95% in Weller et al,27 85.7% in Nandedkar et al18 and specificity values (77% in Al-Dabbagh A, Ibraheem7 and 78% in Weller et al,27 98.6% in Nandedkar et al18).
Overall accuracy of the FNAC system was 92% in the current study. Similar results were reported for the FNAC accuracy by George et al and Periakaruppan et al giving 91% and 93.2% respectively.12,17 These results demonstrate the reliability of the FNAC technique as a predictor of malignancy and assist in clinical decision making.
Statistically significant associations were observed between the Bethesda system of FNAC and TIRADS system of USS, Bethesda system of FNAC and the final histology results. Further, a significant positive correlation was observed between TIRADS system and Bethesda sytem. In keeping with the findings of this study, George et al,12 Vargas-Uricoechea et al28 and have reported similar findings.
Both TIRADS and Bethesda classification systems provide a uniform framework for evaluating thyroid nodules and they facilitate communication among health care professionals. Unless the results are reported by well-trained professionals adhering to the guidelines, interobserver variation can affect the results, leading to limitations in accuracy. Overuse of indeterminate categories has been observed widely in both TIRADS and Bethesda classifications which complicate the interpretation and management of thyroid nodules. Accurate classification of thyroid nodules using TIRADS classification can minimize use of unnecessary invasive procedures like FNAC.28-31
Eventhough, both TIRADS classification and the Bethesda classification system present several limitations that affect the accurate pre-operative diagnosis, findings of the study conclude that cytology reporting by Bethesda system and TIRADS classification of radiology are important preoperative diagnosic tools to identify suspicious thyroid nodules in a setting with limited resources
Recruitment of only patients with radiologically suspected malignancy in the current study was identified as the main limitation that skewed the malignancy rates. Further, not subjecting all the patients to surgeries according to the patient management guidelines was another limitation encountered in the current study that underestimated or overestimated the malignancy rates in certain TIRADS and Bethesda categories.
Study Highlights
What is current knowledge?
-
Thyroid Imaging Reporting and Data System (TIRADS) and Fine Needle Aspiration Cytology (FNAC) reported according to the Bethesda system are internationally accepted preoperative diagnostic tools for thyroid nodules.
-
TIRADS provides a standardized radiological scoring system to estimate malignancy risk, while the Bethesda system offers a cytological framework for risk stratification.
-
Previous studies from high-resource settings have demonstrated variable sensitivity and specificity depending on operator experience and interpretation.
-
Data from low- and middle-income countries (LMICs), particularly on the combined diagnostic performance of TIRADS and FNAC, are scarce.
What is new here?
-
This study is among the first in Sri Lanka to assess the diagnostic performance and concordance of TIRADS and Bethesda systems against histopathology in a resource-limited clinical setting.
-
FNAC (Bethesda system) demonstrated higher specificity (87.5%) and diagnostic accuracy (92%) compared to ultrasound TIRADS (specificity 30.3%, accuracy 70.75%) in predicting thyroid malignancy.
-
A significant positive correlation was observed between higher TIRADS and Bethesda categories and histologically confirmed malignancy.
-
The TIRADS 4c category showed a particularly high malignant risk (87.5%), consistent with international data.
-
Findings highlight that even in resource-limited settings, standardized application of TIRADS and Bethesda systems can improve diagnostic precision, reduce unnecessary surgeries, and optimize preoperative management of thyroid nodules.
Conclusion
FNAC is a robust preoperative diagnostic modality enhances the efficacy when integrated with clinical history and radiological findings. This collaborative improves the determination of thyroid malignancy and optimizes patient care.
Competing Interests
Authors declare that there is no competing of interests.
Ethical Approval
Ethical approval for the study was obtained from the ethics review committee of Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka (65/2019) and informed written consent was taken from each participant of the study.
Acknowledgements
Authors acknowledge Dr. Apsara Epa, Consultant Radiologist, Colombo South Teaching Hospital, Kalubowila, Sri Lanka
References
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 2006; 295(18):2164-7. doi: 10.1001/jama.295.18.2164 [Crossref] [ Google Scholar]
- Mu C, Ming X, Tian Y, Liu Y, Yao M, Ni Y. Mapping global epidemiology of thyroid nodules among general population: a systematic review and meta-analysis. Front Oncol 2022; 12:1029926. doi: 10.3389/fonc.2022.1029926 [Crossref] [ Google Scholar]
- Jayarajah U, Fernando A, Prabashani S, Fernando EA, Seneviratne SA. Incidence and histological patterns of thyroid cancer in Sri Lanka 2001-2010: an analysis of national cancer registry data. BMC Cancer 2018; 18(1):163. doi: 10.1186/s12885-018-4083-5 [Crossref] [ Google Scholar]
- Mazeh H, Mizrahi I, Halle D, Ilyayev N, Stojadinovic A, Trink B. Development of a microRNA-based molecular assay for the detection of papillary thyroid carcinoma in aspiration biopsy samples. Thyroid 2011; 21(2):111-8. doi: 10.1089/thy.2010.0356 [Crossref] [ Google Scholar]
- Nguyen QT, Lee EJ, Huang MG, Park YI, Khullar A, Plodkowski RA. Diagnosis and treatment of patients with thyroid cancer. Am Health Drug Benefits 2015; 8(1):30-40. [ Google Scholar]
- Horvath E, Majlis S, Rossi R, Franco C, Niedmann JP, Castro A. An ultrasonogram reporting system for thyroid nodules stratifying cancer risk for clinical management. J Clin Endocrinol Metab 2009; 94(5):1748-51. doi: 10.1210/jc.2008-1724 [Crossref] [ Google Scholar]
- Al-Dabbagh A, Ibraheem MM. Clinical, cytological and histological correlation of thyroid nodule (S): an observation study. Kirkuk J Med Sci 2021; 7(1):61-70. doi: 10.32894/kjms.2021.169391 [Crossref] [ Google Scholar]
- Krišto B, Vidović Krželj I, Krželj A, Perković R. Ultrasound guided fine needle aspiration cytology (FNAC): an assessment of the diagnostic potential in histologically proven thyroid nodules. Med Glas (Zenica) 2022; 19(2):184-8. doi: 10.17392/1469-22 [Crossref] [ Google Scholar]
- Kumar SK, Seetharamaiah T, Rampure D, Ramakrishna C, Devi RY. Thyroid nodule: cytohistological correlation. Sch J Appl Med Sci 2013; 1(6):745-7. doi: 10.36347/sjams.2013.v01i06.0021 [Crossref] [ Google Scholar]
- Brix TH, Knudsen GP, Kristiansen M, Kyvik KO, Orstavik KH, Hegedüs L. High frequency of skewed X-chromosome inactivation in females with autoimmune thyroid disease: a possible explanation for the female predisposition to thyroid autoimmunity. J Clin Endocrinol Metab 2005; 90(11):5949-53. doi: 10.1210/jc.2005-1366 [Crossref] [ Google Scholar]
- Li R, Wang Y, Du L. A rapidly increasing trend of thyroid cancer incidence in selected East Asian countries: joinpoint regression and age-period-cohort analyses. Gland Surg 2020; 9(4):968-84. doi: 10.21037/gs-20-97 [Crossref] [ Google Scholar]
- George NA, Suresh S, Jiji V, Renu S, Thomas S, Janardhan D. Correlation of TIRADS and Bethesda scoring systems with final histopathology of thyroid nodules–an institutional experience. Indian J Otolaryngol Head Neck Surg 2022; 74(Suppl 3):5753-8. doi: 10.1007/s12070-021-02380-8 [Crossref] [ Google Scholar]
- Fernández Sánchez J. TI-RADS classification of thyroid nodules based on a score modified regarding the ultrasound criteria for malignancy. Rev Argent Radiol 2014; 78(3):138-48. doi: 10.1016/j.rard.2014.07.015 [Crossref] [ Google Scholar]
- De D, Dutta S, Tarafdar S, Kar SS, Das U, Basu K. Comparison between sonographic features and fine needle aspiration cytology with histopathology in the diagnosis of solitary thyroid nodule. Indian J Endocrinol Metab 2020; 24(4):349-54. doi: 10.4103/ijem.IJEM_349_20 [Crossref] [ Google Scholar]
- Kwak JY, Han KH, Yoon JH, Moon HJ, Son EJ, Park SH. Thyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer risk. Radiology 2011; 260(3):892-9. doi: 10.1148/radiol.11110206 [Crossref] [ Google Scholar]
- Srinivas MN, Amogh VN, Gautam MS, Prathyusha IS, Vikram NR, Retnam MK. A Prospective Study to Evaluate the Reliability of Thyroid Imaging Reporting and Data System in Differentiation between Benign and Malignant Thyroid Lesions. J Clin Imaging Sci 2016; 6:5. doi: 10.4103/2156-7514.177551 [Crossref] [ Google Scholar]
- Periakaruppan G, Seshadri KG, Vignesh Krishna GM, Mandava R, Sai VP, Rajendiran S. Correlation between ultrasound-based TIRADS and Bethesda system for reporting thyroid-cytopathology: 2-year experience at a tertiary care center in India. Indian J Endocrinol Metab 2018; 22(5):651-5. doi: 10.4103/ijem.IJEM_27_18 [Crossref] [ Google Scholar]
- Nandedkar SS, Dixit M, Malukani K, Varma AV, Gambhir S. Evaluation of thyroid lesions by fine-needle aspiration cytology according to bethesda system and its histopathological correlation. Int J Appl Basic Med Res 2018; 8(2):76-82. doi: 10.4103/ijabmr.IJABMR_169_17 [Crossref] [ Google Scholar]
- Zhu Y, Song Y, Xu G, Fan Z, Ren W. Causes of misdiagnoses by thyroid fine-needle aspiration cytology (FNAC): our experience and a systematic review. Diagn Pathol 2020; 15(1):1. doi: 10.1186/s13000-019-0924-z [Crossref] [ Google Scholar]
- Jo VY, Stelow EB, Dustin SM, Hanley KZ. Malignancy risk for fine-needle aspiration of thyroid lesions according to the Bethesda System for Reporting Thyroid Cytopathology. Am J Clin Pathol 2010; 134(3):450-6. doi: 10.1309/ajcp5n4mthpafxfb [Crossref] [ Google Scholar]
- Weller A, Sharif B, Qarib MH, St Leger D, De Silva HS, Lingam RK. British Thyroid Association 2014 classification ultrasound scoring of thyroid nodules in predicting malignancy: diagnostic performance and inter-observer agreement. Ultrasound 2020; 28(1):4-13. doi: 10.1177/1742271x19865001 [Crossref] [ Google Scholar]
- Katoh H, Yamashita K, Enomoto T, Watanabe M. Classification and general considerations of thyroid cancer. Ann Clin Pathol 2015; 3(1):1045. [ Google Scholar]
- Cossu A, Budroni M, Paliogiannis P, Palmieri G, Scognamillo F, Cesaraccio R. Epidemiology of thyroid cancer in an area of epidemic thyroid goiter. J Cancer Epidemiol 2013; 2013:584768. doi: 10.1155/2013/584768 [Crossref] [ Google Scholar]
- Miranda-Filho A, Lortet-Tieulent J, Bray F, Cao B, Franceschi S, Vaccarella S. Thyroid cancer incidence trends by histology in 25 countries: a population-based study. Lancet Diabetes Endocrinol 2021; 9(4):225-34. doi: 10.1016/s2213-8587(21)00027-9 [Crossref] [ Google Scholar]
- Chaigneau E, Russ G, Royer B, Bigorgne C, Bienvenu-Perrard M, Rouxel A. TIRADS score is of limited clinical value for risk stratification of indeterminate cytological results. Eur J Endocrinol 2018; 179(1):13-20. doi: 10.1530/eje-18-0078 [Crossref] [ Google Scholar]
- Dy JG, Kasala R, Yao C, Ongoco R, Mojica DJ. Thyroid Imaging Reporting and Data System (TIRADS) in Stratifying Risk of Thyroid Malignancy at The Medical City. J ASEAN Fed Endocr Soc 2017; 32(2):108-16. doi: 10.15605/jafes.032.02.03 [Crossref] [ Google Scholar]
- Weller A, Sharif B, Qarib MH, St Leger D, De Silva HS, Lingam RK. British Thyroid Association 2014 classification ultrasound scoring of thyroid nodules in predicting malignancy: Diagnostic performance and inter-observer agreement. Ultrasound 2020; 28(1):4-13. doi: 10.1177/1742271x19865001 [Crossref] [ Google Scholar]
- Vargas-Uricoechea H, Meza-Cabrera I, Herrera-Chaparro J. Concordance between the TIRADS ultrasound criteria and the BETHESDA cytology criteria on the nontoxic thyroid nodule. Thyroid Res 2017; 10:1. doi: 10.1186/s13044-017-0037-2 [Crossref] [ Google Scholar]
- Russ G, Trimboli P, Buffet C. The new era of TIRADSs to stratify the risk of malignancy of thyroid nodules: strengths, weaknesses and pitfalls. Cancers (Basel) 2021; 13(17):4316. doi: 10.3390/cancers13174316 [Crossref] [ Google Scholar]
- Evranos B, Polat SB, Baser H, Ozdemir D, Kilicarslan A, Yalcin A. Bethesda classification is a valuable guide for fine needle aspiration reports and highly predictive especially for diagnosing aggressive variants of papillary thyroid carcinoma. Cytopathology 2017; 28(4):259-67. doi: 10.1111/cyt.12384 [Crossref] [ Google Scholar]
- Ludvíková M, Kholová I. [Up-to-date experience with the international classification system Bethesda 2010 for thyroid fine-needle aspirate: a review]. Cesk Patol 2014;50(3):155-60. [Czech].