J Res Clin Med. 13:34767.
doi: 10.34172/jrcm.025.34767
Review Article
An overview on recent developments in insulin pump therapy with a regional perspective
Faatimah Maryam Muzammil Conceptualization, Project administration, Resources, Writing – review & editing, , * 
Hafsah Shehzad Investigation, Visualization, Writing – original draft, Writing – review & editing,
Sadia Rounak Shriya Data curation, Methodology, Supervision, Writing – review & editing,
Tasnima Tayb Investigation, Methodology, Writing – original draft, Writing – review & editing,
Yusra Iqbal Data curation, Resources, Validation, Writing – review & editing,
Ali El Houni Project administration, Supervision, Validation, Writing – review & editing,
Author information:
Dubai Medical College for Girls, Dubai, U.A.E.
Abstract
Insulin therapy is vital for managing elevated glucose levels among patients with type 1 diabetes and some individuals with type 2 diabetes. A drawback in traditional methods of insulin administration, including syringes and pens, lies in their limited effectiveness, mainly due to improper storage and poor patient adherence. Furthermore, the invasive nature of these traditional modalities contributes to the observed challenges in patient adherence. By using insulin pumps, clinicians and patients can achieve more consistent and improved euglycemic control. This paper summarizes knowledge and research through a comprehensive literature review. Through our research, we want to highlight the various recent advancements in insulin pump therapy. We hope this paper contributes significantly to understanding new technologies and moves us closer to making insulin pump therapy more accessible.
Keywords: Diabetes mellitus, Glycemic index, Insulin infusion systems
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
There was no funding for this study.
Introduction
The World Health Organization (WHO) estimates that 422 million people around the world have diabetes, with 150 to 200 million of those taking insulin – thereby highlighting the importance of effective insulin administration techniques.1 The insulin pump is one such example. Insulin management utilizing insulin pump therapies has demonstrated notable efficiency, adaptability, and a positive association with improved glycemic outcomes. Since their introduction nearly 50 years ago, insulin pumps have undergone substantial technological enhancements, rendering them more flexible, compact, precise, and reliable than ever before.2 Diabetes is widely recognized as a major public health concern, presenting challenges for the healthcare systems and requiring innovative solutions to improve quality of life.3 This update explores the available insulin pump utilization and provides valuable insights that can inform healthcare policies, clinical practices, and diabetes management strategies tailored to the needs of this region’s diverse population. The article discusses the latest clinical developments in insulin pump therapy for both type 1 and type 2 diabetes mellitus.
Methods
This review provides an overview of recent trends in development in insulin therapy and related patient care in the Middle East. Articles were selected from EBSCO, PubMed, SpringerLink, Sage Journals, American Diabetes Association, BMJ, NEJM, Frontiers and The Lancet. We used a combination of keywords – “Diabetes Mellitus”, “Insulin pump,” “Recent advancements,” “latest updates”, “CSII”, and “Regional overview” –to shortlist articles for detailed review. More than 20 articles were excluded due to duplicated information, irrelevance to our focused study region and non-English content. By primarily focusing on studies from 2010–2023, around 40 articles were finalized based on relevancy of local and regional-based perspectives and latest studies. Qualitative and quantitative data pertaining to trends in insulin pump development were studied over September–December 2023 and verified through expert guidance.
Results
The comprehensive literature review conducted in this overview provides valuable insights into insulin pump therapy, with a focus on different methods. The key findings and trends identified are summarized below.
Recently, blood glucose control has been transformed by automated insulin delivery systems in the form of an ’artificial pancreas’ in a hybrid closed-loop system with further incorporation of a dual-hormone pump.4 Further innovation is focused on achieving a fully automated pancreas with the help of AI through reinforcement learning (RL) design.5 New continuous glucose monitoring (CGM) sensors that can be implanted for up to 90 days are being implemented to reduce significant cost and management.6 The most recent ease of usage is hoped by the Food and Drug Administration (FDA) approved Bionic Pancreas pump that requires minimal user input.7 Finally, diabetes device “interoperability” is being explored with the latest rise of the “Do-It-Yourself” phenomenon.8
Discussing further into the recent advancements, below we have highlighted the most prominent insulin pump therapies that have come into light recently.
Continuous Subcutaneous Insulin Infusion System
The continuous subcutaneous insulin infusion (CSII) administration system has demonstrated notable capabilities. The CSII system is designed to mimic the complex patterns of physiological insulin secretion typically seen in a healthy pancreas. This emulation aims to maintain insulin levels within a range that mirrors those naturally observed in non-diabetic individuals.4
It helps the occurrence of hypoglycemia by carefully modulation insulin delivery. Moreover, this system plays a pivotal role in the maintenance of HbA1c levels which is achieved by mitigating postprandial glucose peaks and minimizing overall glycemic variability, attributed to the utilization of rapid-acting insulin formulations.9
Furthermore, the integration facilitates the downloading of this data, enabling users to engage in comprehensive analysis, thereby empowering them to make informed diabetes management decisions.9
In a study, CSII therapy in comparison to multiple daily insulin injections (MDI) showed significantly lower HbA1c-7.3% (6.6-8.0%) vs 8.2% (7.2-9.6%) (P < 0.0001), lower coefficient of variation (CV) 27.2% ( ± 9.8) vs 34.7% ( ± 11.3) (P < 0.0001), fewer hypoglycemia episodes (P < 0.0001).10
Sensor Augmented Pump Therapy
The sensor augmented pump (SAP) is a combination of CGM technology and CSII. The CGM device is primarily made of a sensor, transmitter and receiver.
The sensor is a thin, flexible tube that is inserted in the subcutaneous tissue and continuously measures glucose levels in the interstitial fluid. The transmitter is responsible for sending the glucose data to the receiver which displays the glucose values.
In an SAP system, the insulin pump pairs to a CGM system and displays the glucose measurements on the pump’s home screen. This allows users easy access to the sensor glucose information.4
Using the glucose sensor capable of continuous blood glucose measurement at frequent intervals is highly beneficial. It gives the clinicians and patients more insight into the blood glucose levels at different times of the day, while doing different activities which can reduce the incidence of hypoglycemic episodes.
The multicenter Real Trend study, as illustrated in Figure 1,11 highlights the advantages of using SAP over traditional CSII. The study consisted of patients who previously had inadequate glycemic control. On SAP therapy, their glycemic control improved –it was specifically noted that the HbA1c levels improved by 1.23% over six months for the 91 patients who wore the sensor ≥ 70% of the time, and by 1.14% for all patients (n = 115). In contrast, the CSII group saw only a 0.55% improvement.12
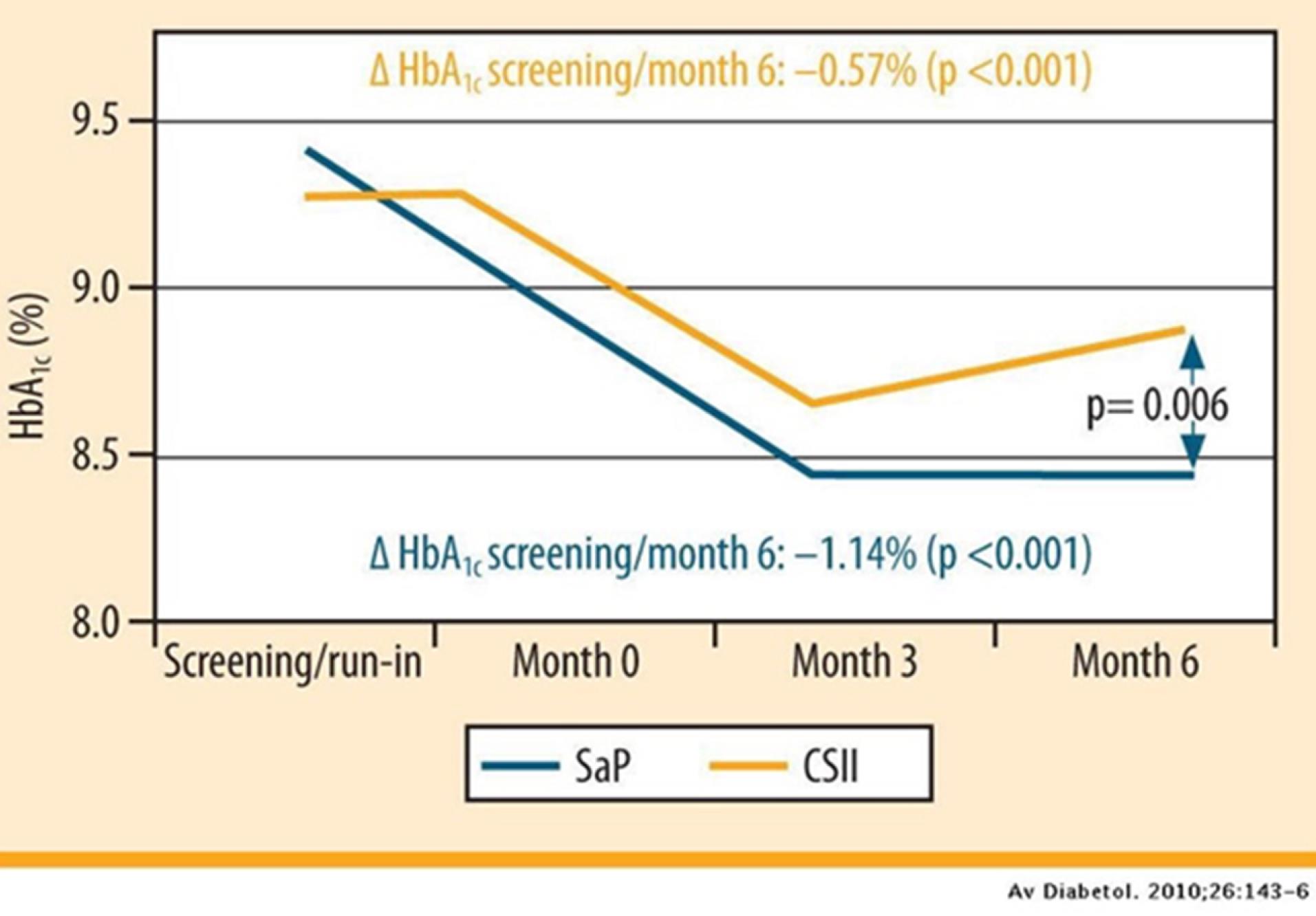
Figure 1.
HbA1c trend in patients, wearing the sensor ≥ 70% of the time
.
HbA1c trend in patients, wearing the sensor ≥ 70% of the time
In another 6-month observational study conducted in Japan in patients with type 1 diabetes the utilization of SAP therapy was associated with a decrease in HbA1c trends, an increase in the proportion of patients with Time in Range (TIR) > 70% and/or Time above range (TAR) < 25%, better satisfaction with treatment, and a decrease in the Clarke score.13
Insulin Pumps with Hypoglycemia Suspension
Advances in SAP technology have enabled the development of hypoglycemia suspension systems through the seamless integration with CGM devices.
The inaugural model to incorporate such functionality was the MiniMed 530G. It releases insulin in response to hypoglycemia occurrences. This initial feature is known as “threshold suspend” or “low glucose suspend” (LGS). Studies and research using LGS revealed a noteworthy 40%–50% reduction in instances of hypoglycemia ( < 70 mg/dL). This was achieved without any discernible increase in A1C levels or mean sensor glucose values when contrasted with SAP therapy alone.4
This technology shows that integrating insulin pumps with low glucose suspension reduced nocturnal hypoglycemia in those at greatest risk and was well accepted by patients.13
These systems function by collecting data via CGM, and cause insulin delivery 30 minutes before hypoglycemia is predicted to occur. These technologies have proved extremely effective in reducing nocturnal hypoglycemia by demonstrating a 50%–80% reduction in hypoglycemia overnight, without increasing the risk of ketosis, and an overall 31%–50% reduction in hypoglycemia when using predictive low glucose suspends (PLGS) compared to SAP alone, with no increase in mean glucose value or hyperglycemia.4
Newer technologies and systems have also evolved – the MiniMed 670G and non-automated pump and sensor systems. Both technologies work on the principle of PLGS.
Closed Loop Insulin Pump
Closed-loop insulin pumps, dubbed as “artificial pancreas”, bridge CGM and insulin infusion through advanced algorithms that facilitate automated delivery. Artificial pancreas systems can be categorized into six types based on their level of automation as shown in Figure 214: Low-Glucose Suspend system, Hypoglycemia minimizer, Hypo/hyperglycemia minimizer, Hybrid closed loop, fully automated insulin closed loop and finally, fully automated multihormone closed loop.14
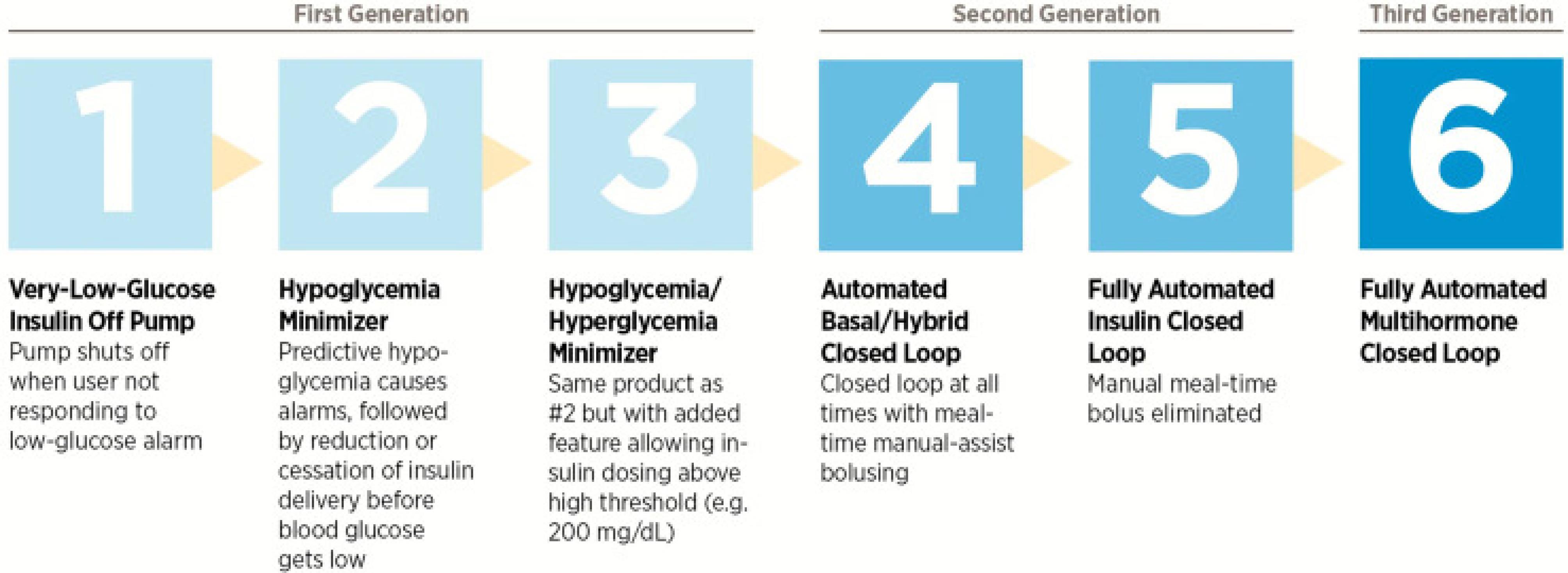
Figure 2.
The six categories of closed-loop systems as defined by the Juvenile Diabetes Research Foundation
.
The six categories of closed-loop systems as defined by the Juvenile Diabetes Research Foundation
When Medtronic commercialized MiniMed Paradigm Veo, the first LGS system in 2009, the simple closed-loop system was better than sensor-augmented pump therapy to reduce nocturnal hypoglycemia.15 Low-glucose pump automatically suspend insulin delivery in response to low glucose levels up to a certain threshold, without requiring user confirmation. Later in 2016, Medtronic successfully released MiniMed 670G – the first commercially available Hybrid Closed Loop. In comparison to fully closed-loop systems, a more advanced type of artificial pancreas, the hybrid system requires users to manually program insulin boluses with meals. Hybrid-closed loops showed greater reductions in HbA1c, hyperglycemia and hypoglycemia compared to baseline in an analysis of 124 adults and adolescents using the system at home. It was shown that adolescent HbA1c levels decreased from 7.7% ± 0.8% to 7.1% ± 0.6% (P< 0.001) and adults HbA1c levels from 7.3% ± 0.9% to 6.8% ± 0.6%.16
In contrast, fully closed-loop systems are designed to automate hormone delivery entirely, eliminating the need for user input for mealtime boluses. However, there are two main challenges: (i) control of postprandial hyperglycemia in the absence of user input of carbohydrate content of meals and (ii) control of exercise-induced hypoglycemia in absence of user-input for duration, type and intensity of exercise. For control of postprandial hyperglycemia, innovators are designing algorithms to estimate carbohydrate levels based on either minimal input such as the iLet’s Bionic Pancreas17 or integration of a smartphone application that uses images submitted by users to calculate carbohydrate content.18
To overcome exercise-induced effects, trials are on-going to create algorithms that use user’s heart rate, temperature, acceleration to determine biometric data for type and intensity of exercise.19
Due to afore mentioned challenges, only one commercial fully closed system is available in Japan called STG-55; however, these are other bedside devices that are available.20
Dual hormone closed loop systems are able to administer boluses glucagon along with insulin infusion. Glucagon is more effective in preventing hypoglycemia than suspending insulin due to its relatively rapid onset (5 minutes) compared to rapid-acting insulin (15 minutes).21 Dual hormone closed-loop has been shown to result in increased time in target as compared to single-hormone closed loop system in a meta-analysis conducted in 2017.22 However, until recently, the solvent stability of glucagon was a limiting factor.23
A new approach towards dual-hormone closed-loop algorithm is incorporation of insulin-pramlintide coformulation in tackling postprandial glucose levels has shown better postprandial control and improvement in daytime glycemic control.24,25 Pramlintide is a pancreatic hormone that delays gastric emptying and inhibits glucagon secretion. Although insulin-pramlintide closed loop systems require two separate infusion reservoirs, trials are ongoing to better this approach.26
Finally, diabetes device “interoperability” is being explored with the latest rise of the “Do-It Yourself” DIY phenomenon. Initiated in 2013 under the hashtag of #WeAreNotWaiting, the diabetic community collaborated to create open-sourced closed loop software. By connecting commercially available insulin pumps to open-source algorithms, users gained more control and flexibility to design devices that were tailored to the user.27
Table 1 provides an overview of various frequently seen insulin pump models with their respective modes of action.
Table 1.
Insulin pump devices and their mode of action
|
Devices
|
Mode of action
|
| MiniMedTM 780G system |
Hybrid closed-loop approach |
| Tandem t:slim X2 pump (standalone system) |
Advanced Hybrid Closed-Loop Technology with or without Control-IQ |
| Dexcom G6 |
Dexcom G6 Continuous Glucose Monitoring system relies on a subcutaneous glucose oxidase-based sensor that is factory calibrated and allows for optional user-initiated calibrations. |
| Flash glucose monitoring with FreeStyle Libre 2 (FSL2) |
Continuous glucose monitoring system developed by Abbott |
| The Omnipod DASHTM Insulin Management System |
Continuous Glucose Monitoring system on tubeless pump system |
| EOPatch Insulin Pump |
Patch pump |
Insulin Pumps: for Type 2 Diabetes Mellitus
The majority of the existing options of insulin pumps cater to the demands of individuals with T1DM (type 1 diabetes mellitus). These pumps monitor various things and have advanced features which might not be necessary in patients with T2DM.
Additionally, the requirement of complex features and educational approach required to understand the advanced features may deter individuals from using CSII eventually leading to underutilization of the current pump system.
Table 2 represents the pumps available for use in T2DM patients.28
Table 2.
Insulin pumps designed specifically for patients with T2DM
|
|
V-Go
|
PaQ
|
Simplicity
|
| Manufacturer |
Valeritas |
CeQur |
CeQur |
| Intended for |
T2DM |
T2DM |
T1DM + T2DM |
| Kind of pump |
Patch pump |
Patch pump |
Bolus patch pump |
| Basal rate |
Three pump models with pre-set basal rate profiles (20, 30, or 40 U/d) |
Seven pre-set profiles (16, 20, 24, 32, 40, 50, and 60 U/d) |
None |
| Bolus types |
2 U increments |
2 U increments |
2 U increments |
| Insulin reservoir |
56 U (V-Go 20)
66 U (V-Go 30)
76 U (V-Go 40) |
330 U |
200 U |
| Insulin |
U-100 |
U-100 |
U-100 |
| Device use |
Daily replacement |
Multiday device (3 d) |
Multiday device (3 d) |
The V-Go and PaQ systems offer continuous basal insulin delivery, which can help maintain more stable blood sugar levels, especially for people with T2DM who need a consistent background level of insulin throughout the day. They can deliver insulin in small increments (e.g., 2-unit increments) allowing for more precise insulin dosing, which is particularly important for individuals with T2DM who have varying insulin needs based on their daily activities and dietary intake. Further, these systems are fully disposable and do not require complicated maintenance or cleaning. This feature can reduce the burden of insulin management for individuals with T2DM.28
Automated Insulin Delivery Systems and Their Interoperability
As we previously discussed, in addition to insulin pumps, diverse other technological devices like blood glucose meters or CGM systems are now available for patients with diabetes. A study with hospitalized patients with T2DM demonstrated a significant reduction in the time to achieve glucose targets and to decrease exposures to hypo-/hyperglycemia using a SAP compared with MDI therapy.
Recently, the FDA also authorized the first interoperable, automated insulin dosing controller: the Tandem Diabetes Care Control-IQ. Connected to an ACE pump and an integrated CGM, the glycemic controller automatically adjusts basal insulin deliveries. Thus, after the approval of the integrated automated insulin delivery (AID) system MiniMed 670G, the controller represents the first stand-alone interoperable automated glycemic controller.
The possibility to connect other devices is currently not given by simple patch pumps specifically intended for patients with T2DM. However, the use of AID systems may simplify treatment for both patients and caregivers in inpatient settings. An improved time in range without increased risk of hypoglycemia when using an AID system compared to usual care has already been demonstrated in inpatients with T2DM. Additionally, high system acceptability was reported, and most patients were pleased to have managed their glucose control autonomously.28
Regional Overview of Insulin Pump Therapy in the Middle East
In a multicenter prospective study conducted in UAE, which included 38 participants, the use of insulin pump therapy in patients with type 1 diabetes was observed. In this study, two primary parameters were noted treatment and patient satisfaction. These were recorded initially at baseline, and then at further visits of around 12 and 24 weeks. The study revealed that the use of a pump system with remote control led to an overall improvement in HbA1c levels and patient satisfaction. The mean decrease in the levels of HbA1c was noted to be around 1.09% with a P= 0.00009, in the primary group wherein the mean age of the participants was 16 years and 0.79% (P = 0.09) for the second group with a mean age of 9 years.5
In another 6-month prospective study conducted from 2014-2015 in Saudi Arabia, 47 patients (age 17-24) with type 1 diabetes were selected. These individuals regularly attended the Insulin Pump Clinic at Prince Sultan Military Medical City, Riyadh. Compared to baseline, improvements and positive satisfaction were observed in patients after 6 months. The frequency of hyperglycemia and hypoglycemia episodes had declined significantly. Patients with long-standing type T1DM showed a significant decline in insulin requirement at 6 months when compared to baseline.29
In a retrospective and cross-sectional study conducted in Qatar in 2018, CSII characteristics and results were observed in 138 patients among children and adolescents. The results of the study as shown in Figure 330 noted that HbA1c levels were reduced by an average of around 1.6% (17.5 mmol/mol). This occurred over a time duration of one year and was observed with various insulin pump models. An average level of HbA1c at around 7.7% was seen among patients who utilized the sensor-augmented pump alongside the PLGS at the end of the study.30
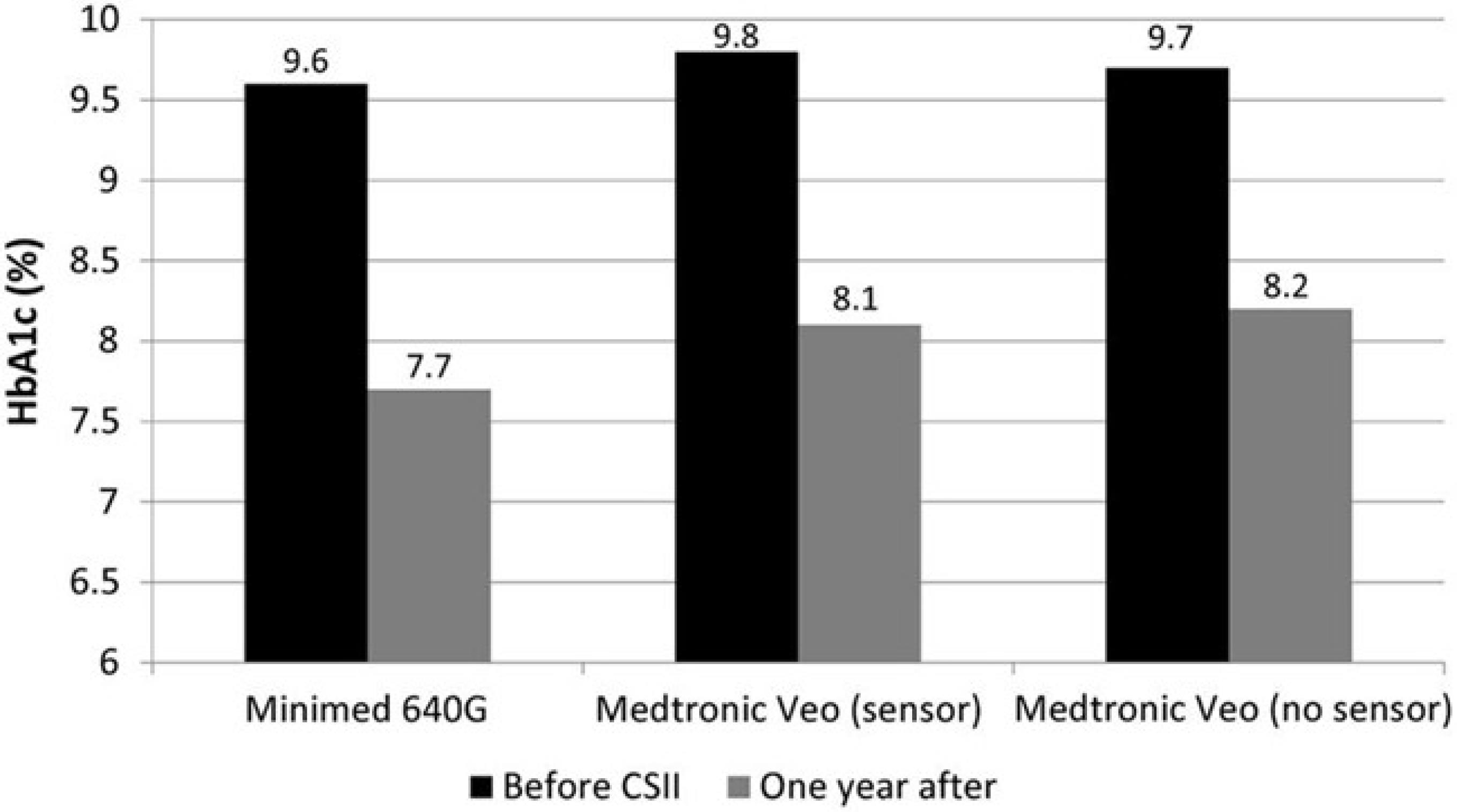
Figure 3.
HbA1c levels based on the type of CSII insulin pump used in Qatar
.
HbA1c levels based on the type of CSII insulin pump used in Qatar
However, knowledge and aptitude of physicians in the Middle Eastern Region should arise to reflect the advancements. The Kingdom of Saudi Arabia (KSA) ranks ninth out of the top ten countries with the highest incidence of T1DM per year as per the Diabetes Atlas (9th edition). Yet a study showed that of 300 physicians in Saudi Arabia, 56.7% had poor knowledge level, while 53.4% had positive attitude.31 Specialization, years of practice and older age were key factors in influencing aptitude. Another similar study highlights this need where the majority of responses of healthcare providers (80%) did not know the basic components of insulin pump and 79% did not know that insulin pump can be loaded with insulin by the patients themselves based on their need.32
Discussion
Insulin pumps were marketed first in the early 1970s and had undergone rapid development in the last fifty years. The landmark Diabetes Control and Complications Trial (DCCT) was one of the factors that led to its rapid growth.33 According to the most recent statistics, there are now over 1 million people with diabetes who are using insulin pumps.34
Insulin pump therapy has greatly advanced the day-to-day lifestyle. By enabling greater lifestyle flexibility, improved glucose management, and fewer complications, insulin pumps have significantly enhanced quality of life. Furthermore, the novel closed loop insulin pumps are hoped to be relatively cost-effective compared to the continued use of CSII in people with T1DM; while for people with T2D simple insulin infusion devices such as PAQ® have the potential to be highly cost-effective.35,36
However, challenges remain in terms of psychosocial, financial and technological barriers. Previous studies and meta-analyses investigated the topic of psychosocial issues related to insulin pump users.37-39 Considerations to discontinue pump usage were not limited to finance or logistics, but technological frustrations, wear-related issues, unmet glycemic and workload expectations contributed to discontinuation. Therefore, clinicians should evaluate a patient’s willingness and ability to consistently use and maintain an insulin pump.
Since most insulin pump users have type 1 diabetes, children, teens and adolescents tend to be self-conscious about their body image and wearing an insulin pump continuously might affect their mental health. Moreover, the initial pump setup is noticeably complicated for children, and thereby appropriate counseling must be provided to parents regarding device operation.40
Older adults face distinct challenges in continuing insulin pump therapy. Timely access to equipment and regular follow-up appointments every 3 months were significant challenges. Both these reasons led to patients deterring appointments, attempting to use alternative methods of delivery such as injections, or stopping the usage of insulin for a period which increased the risk of adverse complications such as diabetic ketoacidosis (DKA).41 Additionally, older individuals are prone to develop conditions which impact their dexterity – for example in patients who have weakness in one limb for e.g., after stroke, or patients with osteoarthritis, sensory loss, etc. might face difficulty with intact dexterity which would affect effective insulin pump therapy. These issues present ongoing challenges that modern medicine must address.
From our systematic review, there are several options available for clinicians and patients with diabetes irrespective of age or the type of diabetes. Certain challenges such as education, device wear, self-care, clinical follow-ups must be addressed by clinicians and all available help should be provided to overcome them.
Study Highlights
What is current knowledge?
What is new here?
-
This paper reviews the latest advancements in insulin pump therapy for type 1 and type 2 diabetes with an emphasis on Middle East. It highlights that these innovations can improve accessibility, guide future healthcare strategies, and enhance patient care.
Conclusion
In summary, this overview manuscript has provided a comprehensive survey of insulin pump therapy, offering valuable insights into its modes of operation, clinical outcomes, and emerging trends. We have observed the continuous progression of insulin pump technology, and the potential they hold in optimizing glycemic control. The clinical benefits, including improved HbA1c levels and reduced hypoglycemia highlight the importance of these devices in enhancing the quality of life for individuals with diabetes.
Considering the several novel innovations and technologies in insulin pumps, there is still limited data availability and further larger randomized controlled trials with more patients and for larger periods of time may be needed.
As Insulin pumps continue to evolve, it is imperative that healthcare professionals, researchers and policy makers collaborate to address any challenges and promote equitable access. It is our hope that this overview contributes to the collective understanding of this vital aspect of diabetes care and inspires further advancements in the field.
Competing Interests
All authors declare no competing interests.
Ethical Approval
Not applicable.
Acknowledgements
We would like to thank Almighty for giving us the direction and ability to complete this research. We also extend our gratitude to all the authors who wrote the articles we reviewed.
References
- World Health Organization (WHO). Diabetes. WHO; 2023.
- Heinemann L, Fleming GA, Petrie JR, Holl RW, Bergenstal RM, Peters AL. Insulin pump risks and benefits: a clinical appraisal of pump safety standards, adverse event reporting, and research needs: a joint statement of the European Association for the Study of Diabetes and the American Diabetes Association Diabetes Technology Working Group. Diabetes Care 2015; 38(4):716-22. doi: 10.2337/dc15-0168 [Crossref] [ Google Scholar]
- Sugandh F, Chandio M, Raveena F, Kumar L, Karishma F, Khuwaja S. Advances in the management of diabetes mellitus: a focus on personalized medicine. Cureus 2023; 15(8):e43697. doi: 10.7759/cureus.43697 [Crossref] [ Google Scholar]
- Berget C, Messer LH, Forlenza GP. A clinical overview of insulin pump therapy for the management of diabetes: past, present, and future of intensive therapy. Diabetes Spectr 2019; 32(3):194-204. doi: 10.2337/ds18-0091 [Crossref] [ Google Scholar]
- Deeb A, Akle M, Abdulrahman L, Suwaidi H, Awad S, Remeithi S. Using insulin pump with a remote-control system in young patients with diabetes improves glycemic control and enhances patient satisfaction. Clin Diabetes Endocrinol 2019; 5:7. doi: 10.1186/s40842-019-0081-z [Crossref] [ Google Scholar]
- Choudhary P, Shin J, Wang Y, Evans ML, Hammond PJ, Kerr D. Insulin pump therapy with automated insulin suspension in response to hypoglycemia: reduction in nocturnal hypoglycemia in those at greatest risk. Diabetes Care 2011; 34(9):2023-5. doi: 10.2337/dc10-2411 [Crossref] [ Google Scholar]
- Nauck MA, Kahle-Stephan M, Lindmeyer AM, Wenzel S, Meier JJ. Prediction of individual basal rate profiles from patient characteristics in type 1 diabetes on insulin pump therapy. J Diabetes Sci Technol 2021; 15(6):1273-81. doi: 10.1177/1932296820972691 [Crossref] [ Google Scholar]
- Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366:l4898. doi: 10.1136/bmj.l4898 [Crossref] [ Google Scholar]
- Callahan Fagan VR, Parsons K. The lived experience of continuous subcutaneous insulin infusion in adults with type 1 diabetes mellitus: a phenomenological inquiry. Glob Qual Nurs Res 2021; 8:2333393620981058. doi: 10.1177/2333393620981058 [Crossref] [ Google Scholar]
- Tsarkova P, Chakarova N, Dimova R, Grozeva G, Todorova A, Serdarova M. CSII is related to more stable glycemia in adults with type 1 diabetes. Endocrine 2022; 75(3):776-80. doi: 10.1007/s12020-021-02913-9 [Crossref] [ Google Scholar]
- Schönauer M, Thomas A. Sensor-augmented pump therapy – on the way to artificial pancreas. Avances Diabetol 2010; 26(3):143-6. doi: 10.1016/S1134-3230(10)63002-5 [Crossref] [ Google Scholar]
- Weinzimer SA, Tamborlane WV. Sensor-augmented pump therapy in type 1 diabetes. Curr Opin Endocrinol Diabetes Obes 2008; 15(2):118-22. doi: 10.1097/MED.0b013e3282f7960b [Crossref] [ Google Scholar]
- Takagi S, Miura J, Shimura K, Hoshina S, Tsuchida Y, Takita M. A sensor augmented pump may improve awareness of hypoglycemia and quality of life in Japanese patients with type 1 diabetes mellitus. Diabetol Int 2022; 13(1):280-7. doi: 10.1007/s13340-021-00538-x [Crossref] [ Google Scholar]
- Templer S. Closed-loop insulin delivery systems: past, present, and future directions. Front Endocrinol (Lausanne) 2022; 13:919942. doi: 10.3389/fendo.2022.919942 [Crossref] [ Google Scholar]
- Bergenstal RM, Klonoff DC, Garg SK, Bode BW, Meredith M, Slover RH. Threshold-based insulin-pump interruption for reduction of hypoglycemia. N Engl J Med 2013; 369(3):224-32. doi: 10.1056/NEJMoa1303576 [Crossref] [ Google Scholar]
- Garg SK, Weinzimer SA, Tamborlane WV, Buckingham BA, Bode BW, Bailey TS. Glucose outcomes with the in-home use of a hybrid closed-loop insulin delivery system in adolescents and adults with type 1 diabetes. Diabetes Technol Ther 2017; 19(3):155-63. doi: 10.1089/dia.2016.0421 [Crossref] [ Google Scholar]
- Food and Drug Administration (FDA). FDA Clears New Insulin Pump and Algorithm-Based Software to Support Enhanced Automatic Insulin Delivery. FDA; 2023.
- Vasiloglou MF, Mougiakakou S, Aubry E, Bokelmann A, Fricker R, Gomes F. A comparative study on carbohydrate estimation: GoCARB vs dietitians. Nutrients 2018; 10(6):741. doi: 10.3390/nu10060741 [Crossref] [ Google Scholar]
- DeBoer MD, Cherñavvsky DR, Topchyan K, Kovatchev BP, Francis GL, Breton MD. Heart rate informed artificial pancreas system enhances glycemic control during exercise in adolescents with T1D. Pediatr Diabetes 2017; 18(7):540-6. doi: 10.1111/pedi.12454 [Crossref] [ Google Scholar]
- Namikawa T, Munekage M, Yatabe T, Kitagawa H, Hanazaki K. Current status and issues of the artificial pancreas: abridged English translation of a special issue in Japanese. J Artif Organs 2018; 21(2):132-7. doi: 10.1007/s10047-018-1019-4 [Crossref] [ Google Scholar]
- Peters TM, Haidar A. Dual-hormone artificial pancreas: benefits and limitations compared with single-hormone systems. Diabet Med 2018; 35(4):450-9. doi: 10.1111/dme.13581 [Crossref] [ Google Scholar]
- Weisman A, Bai JW, Cardinez M, Kramer CK, Perkins BA. Effect of artificial pancreas systems on glycaemic control in patients with type 1 diabetes: a systematic review and meta-analysis of outpatient randomised controlled trials. Lancet Diabetes Endocrinol 2017; 5(7):501-12. doi: 10.1016/s2213-8587(17)30167-5 [Crossref] [ Google Scholar]
- Wilson LM, Jacobs PG, Ramsey KL, Resalat N, Reddy R, Branigan D. Dual-hormone closed-loop system using a liquid stable glucagon formulation versus insulin-only closed-loop system compared with a predictive low glucose suspend system: an open-label, outpatient, single-center, crossover, randomized controlled trial. Diabetes Care 2020; 43(11):2721-9. doi: 10.2337/dc19-2267 [Crossref] [ Google Scholar]
- Sherr JL, Patel NS, Michaud CI, Palau-Collazo MM, Van Name MA, Tamborlane WV. Mitigating meal-related glycemic excursions in an insulin-sparing manner during closed-loop insulin delivery: the beneficial effects of adjunctive pramlintide and liraglutide. Diabetes Care 2016; 39(7):1127-34. doi: 10.2337/dc16-0089 [Crossref] [ Google Scholar]
- Haidar A, Tsoukas MA, Bernier-Twardy S, Yale JF, Rutkowski J, Bossy A. A novel dual-hormone insulin-and-pramlintide artificial pancreas for type 1 diabetes: a randomized controlled crossover trial. Diabetes Care 2020; 43(3):597-606. doi: 10.2337/dc19-1922 [Crossref] [ Google Scholar]
- Riddle MC. Rediscovery of the second β-cell hormone: co-replacement with pramlintide and insulin in type 1 diabetes. Diabetes Care 2020; 43(3):518-21. doi: 10.2337/dci19-0077 [Crossref] [ Google Scholar]
- Ahmed SH, Ewins DL, Bridges J, Timmis A, Payne N, Mooney C. Do-it-yourself (DIY) artificial pancreas systems for type 1 diabetes: perspectives of two adult users, parent of a user and healthcare professionals. Adv Ther 2020; 37(9):3929-41. doi: 10.1007/s12325-020-01431-w [Crossref] [ Google Scholar]
- Freckmann G, Buck S, Waldenmaier D, Kulzer B, Schnell O, Gelchsheimer U. Insulin pump therapy for patients with type 2 diabetes mellitus: evidence, current barriers, and new technologies. J Diabetes Sci Technol 2021; 15(4):901-15. doi: 10.1177/1932296820928100 [Crossref] [ Google Scholar]
- Al Hayek AA, Robert AA, Al Dawish MA, Braham RB, Goudeh HS, Al Sabaan FS. Efficacy of insulin pump therapy on diabetes treatment satisfaction and glycemic control among patients with type 1 diabetes mellitus in Saudi Arabia: a prospective study. Diabetes Ther 2015; 6(2):227-36. doi: 10.1007/s13300-015-0107-1 [Crossref] [ Google Scholar]
- Petrovski G, Al Khalaf F, Hussain K, Campbell J, El Awwa A. Continuous subcutaneous insulin infusion characteristics in type 1 diabetes children and adolescents in Qatar. Diabetes Ther 2018; 9(5):2091-8. doi: 10.1007/s13300-018-0510-5 [Crossref] [ Google Scholar]
- Alaqeel A, Almushaigeh A, Almijmaj M, Almesned R, Alsuhaibani M. Are physicians in Saudi Arabia ready for patients with an insulin pump? An examination of physician knowledge and attitude. Int J Environ Res Public Health 2020; 17(24):9394. doi: 10.3390/ijerph17249394 [Crossref] [ Google Scholar]
- Alghadeer S, Aljuaydi K, Alanazi M, Balkhi E, Alhossan A, Alruthia Y. The attitude and basic knowledge of insulin pump therapy among healthcare providers. Biomed Res 2019; 30(3):446-51. [ Google Scholar]
- Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, Davis M. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329(14):977-86. doi: 10.1056/nejm199309303291401 [Crossref] [ Google Scholar]
- Association of Diabetes Care & Education Specialists. Insulin Pumps L the DCES and Pump Therapy L Danatech. Available from: https://www.adces.org/education/danatech/insulin-pumps/pumps-in-professional-practice/dces’s-and-pump-therapy.
- Roze S, Buompensiere MI, Ozdemir Z, de Portu S, Cohen O. Cost-effectiveness of a novel hybrid closed-loop system compared with continuous subcutaneous insulin infusion in people with type 1 diabetes in the UK. J Med Econ 2021; 24(1):883-90. doi: 10.1080/13696998.2021.1939706 [Crossref] [ Google Scholar]
- Wahlqvist P, Warner J, Morlock R. Cost-effectiveness of simple insulin infusion devices compared to multiple daily injections in uncontrolled type 2 diabetics in the United States based on a simulation model. J Health Econ Outcomes Res 2018; 6(1):84-95. doi: 10.36469/9789 [Crossref] [ Google Scholar]
- Forlenza GP, Messer LH, Berget C, Wadwa RP, Driscoll KA. Biopsychosocial factors associated with satisfaction and sustained use of artificial pancreas technology and its components: a call to the technology field. Curr Diab Rep 2018; 18(11):114. doi: 10.1007/s11892-018-1078-1 [Crossref] [ Google Scholar]
- Rashotte J, Tousignant K, Richardson C, Fothergill-Bourbonnais F, Nakhla MM, Olivier P. Living with sensor-augmented pump therapy in type 1 diabetes: adolescents’ and parents’ search for harmony. Can J Diabetes 2014; 38(4):256-62. doi: 10.1016/j.jcjd.2014.02.002 [Crossref] [ Google Scholar]
- Messer LH, Johnson R, Driscoll KA, Jones J. Best friend or spy: a qualitative meta-synthesis on the impact of continuous glucose monitoring on life with type 1 diabetes. Diabet Med 2018; 35(4):409-18. doi: 10.1111/dme.13568 [Crossref] [ Google Scholar]
- Argento NB, Liu J, Hughes AS, McAuliffe-Fogarty AH. Impact of Medicare continuous subcutaneous insulin infusion policies in patients with type 1 diabetes. J Diabetes Sci Technol 2020; 14(2):257-61. doi: 10.1177/1932296819838292 [Crossref] [ Google Scholar]
- Toschi E, Munshi MN. Benefits and challenges of diabetes technology use in older adults. Endocrinol Metab Clin North Am 2020; 49(1):57-67. doi: 10.1016/j.ecl.2019.10.001 [Crossref] [ Google Scholar]