J Res Clin Med. 13:34744.
doi: 10.34172/jrcm.025.34744
Original Article
A clinico-endoscopic and histopathological correlation in suspected cases of malabsorption: A cross-sectional study
Sargam Dhaliwal Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing, 1 
Mangesh Londhe Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – review & editing, 1
Archana Buch Conceptualization, Data curation, Funding acquisition, Methodology, Supervision, Writing – original draft, Writing – review & editing, 1, *
Charusheela Gore Data curation, Resources, Visualization, Writing – review & editing, 1
Amol Sonyabapu Dahale Resources, Writing – review & editing, 2
Fatehpal Singh Gill Formal analysis, Software, Visualization, Writing – review & editing, 3
Reshma Alexander Formal analysis, Investigation, Validation, Writing – review & editing, 1
Author information:
1Department of Pathology, Dr. D.Y.Patil Medical College, Hospital and Research Center, Dr. D.Y.Patil Vidyapeeth, Pimpri, Pune, India
2Department of Medical Gastroenterology, Dr. D.Y.Patil Medical College, Hospital and Research Center, Dr.D.Y.Patil Vidyapeeth, Pimpri, Pune, India
3Department of Anaesthesiology, Dr. D.Y.Patil Medical College, Hospital and Research Center, Dr. D.Y.Patil Vidyapeeth, Pimpri, Pune, India
Abstract
Introduction:
Malabsorption is a complex medical condition with a diverse range of underlying etiologies posing a diagnostic challenge. The aim of the study was to investigate the correlation between endoscopic findings and histopathological diagnoses in patients with suspected malabsorption syndrome.
Methods:
This cross-sectional study was conducted over 12 months on 160 patients aged 2 to 60 years with chronic diarrhea and nutritional deficiencies. Endoscopic biopsies of the small intestine were performed and reported based on the following parameters including number and site of the biopsy specimens, villous height, and architecture, villous to crypt (V:C) ratio, presence of crypt hyperplasia and intra-epithelial lymphocyte (IEL) count.
Results:
Clinical presentations included chronic diarrhea (41.9%), weakness (12.9%), weight loss (9%), and constipation (2.5%). Endoscopic findings were normal in 49.69% of population. Histopathological examination revealed villous atrophy (18.6%), increased IEL count (16.9%) and crypt hyperplasia (6.2%). Chronic duodenitis was the most common diagnosis (64.4%). Celiac disease (3.1%) and tropical sprue (1.2%) were diagnosed based on specific criteria, emphasizing the need for histopathological confirmation.
Conclusion:
This study highlights the spectrum of histopathological changes in malabsorption and underscores the importance of its correlation with clinical and endoscopic findings. In clinical scenario of malabsorption, endoscopy findings vary from normal to abnormal mucosal morphology. Normal mucosal study may also reveal pathological changes on histopathological evaluation. Hence histopathology remains a crucial step for understanding etiopathogenesis thus helping to streamline the management.
Keywords: Celiac disease, Endoscopy, Histopathology, Malabsorption
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
No sources of funding.
Introduction
Malabsorption has a wide range of clinical implications and manifestations such as celiac disease, autoimmune enteropathy like Immune-dysregulation, Poly-endocrinopathy, enteropathy X-linked syndrome (IPEX), tropical sprue, small intestinal bacterial overgrowth, protein allergy (milk, soy), eosinophilic gastroenteritis, primary intestinal lymphangiectasia, chronic granulomatous disease, infiltrative diseases such as amyloidosis, systemic lupus erythematosus, sarcoidosis, scleroderma, graft vs host diseases, inherited disorders such as microvillous inclusion disease, abetalipoproteinemia and neoplastic disorders such as Waldenstrom’s macroglobulinemia, Gastrointestinal Stromal tumor, Carcinoid syndrome, Multiple Myeloma, lymphoma, leukemia, and metastasis from other primaries like lung, breast.1-3 The two most important ones are celiac disease and tropical sprue.
Due to the vast etiology of malabsorption, forming an accurate diagnosis and identifying the underlying pathology is the biggest challenge. This is because various etiologies of malabsorption present with overlapping signs and symptoms, making clinical distinction difficult.3 Furthermore, the diagnostic process can be more difficult by the subtle or extraintestinal signs of certain conditions, causing malabsorption. Therefore, to get a baseline assessment of the small intestine damage, literature has endorsed the need for combination diagnostic strategy of endoscopy with histological examination.4 One of the most crucial measures in evaluating patients with malabsorption, considered to date, is an endoscopic biopsy of the small intestine with duodenum being the most preferred site.1,3
The usefulness of endoscopy has been reconsidered in light of growing evidence, that non-endoscopic and non-biopsy methods can diagnose adult patients and that endoscopic findings in cases of malabsorption can be nonspecific. In such cases, serological evidence with positive anti-tissue transglutaminase antibodies is considered reliable.5 However, few studies suggest that the positive predictive value and negative predictive value of the population studied and the history of a gluten-free diet can affect the diagnostic efficacy of testing by anti-tissue transglutaminase antibodies.6 Serological testing also has its limitations such that false negative results can be obtained in conditions like IgA deficiency for diagnosing celiac disease.4 Due to this, upper gastrointestinal endoscopy and histopathological analysis with duodenal biopsies is always recommended.7 This study aims to evaluate small intestinal biopsy specimens including duodenum, jejunum, and ileum patients presenting with the symptoms of malabsorption to correlate these histopathological findings with endoscopic features.
Materials and Methods
This was a descriptive cross-sectional observational study, conducted at the Department of Pathology and Department of Gastroenterology at a tertiary care center in western Maharashtra in India for a period of 12 months from July 2022 to July 2023 on a total of 160 patients. Dr. D Y Patil Vidyapeeth institutional ethics committee approval with protocol reversion was obtained and study was done in accordance with the ethical standards. Written informed consent was taken from each patient.
Both male and female patients between the age group of 2 to 60 years, attending the outpatient department of gastroenterology with a chief complaint of chronic diarrhea of small intestinal type, defined as diarrhea of more than one month of duration or with chronic diarrhea and any one of the proven nutritional deficiencies like vitamin A, D, E, K, iron, B12, and folate were included in the study. Patients outside this age group that is < 2 and > 60 years, with a history of any major gastrointestinal surgery, chronic use of nonsteroidal anti-inflammatory drugs (NSAIDS) or antibiotics, with diagnosed polyps or any gastrointestinal malignancies and with a history of Human Immunodeficiency Virus, chronic kidney disease, heart disease, and pregnant females were excluded from the study. An endoscopy was performed in each patient and small intestinal biopsies were obtained for histopathological examination. The endoscopy was interpreted based on these findings: 0) Normal mucosal study/no significant findings, 1) Scalloping/serrated/fissured duodenal folds, 2) Reduced duodenal folds, 3) Atrophy of duodenal folds, 4) Whitish mucosa/lymphangiectasia of duodenum, 5) Duodenitis (erosions/erythema/healed mucosa), 6) Ulcers in ileum, 7) Erythema in ileum, 8) Stricture in ileum, 9) Nodularity in ileum. A total of 160 small intestinal biopsies were analyzed out of which 135 were from duodenum, 24 from ileum and 1 from jejunum. In case of duodenum, the biopsies were taken from the second part of the duodenum as it is the most preferable and specific site.1 All biopsies were of adequate size, ranging from 0.3 to 0.5 cm in length and adequate depth including mucosa and submucosa. Biopsies from multiple sites were not taken due to cost constraints. Each biopsy was fixed in 10 % neutral buffered formalin (pH 7.0-7.4) for approximately 6-8 hours. Grossing of the biopsy was done, and the biopsy was oriented with the luminal side uppermost and then submitted to prepare block according to the protocol followed in the department. Each biopsy section was dehydrated and embedded in melted paraffin wax, after which a block was made. The cutting of the block was done serially on a microtome and the obtained sections were transferred on slides.
Staining of the slides was done with hematoxylin and eosin (H&E). The H&E-stained slides were studied under the microscope by two pathologists and final reporting was done by consensus of both. Blinding of both the pathologists to clinical details and each other’s findings was ensured to avoid bias. The parameters studied on histopathological examination included the number and site of the biopsy specimens, villous height and architecture, villous to crypt (V:C) ratio, presence of crypt hyperplasia, surface enterocytes, brush borders, intra-epithelial lymphocyte (IEL) count, gastric metaplasia, presence of microorganisms, presence of tumor, Brunner’s glands and inflammation and types of inflammatory cells in lamina propria. Villous atrophy was defined as a flattening of the surface due to the intestinal villi’s shortening and blunting. For determining villous atrophy, well-oriented specimens were considered which had 3-4 crypts in a row arranged perpendicularly over the muscularis mucosa with overlying 4-5 consecutive elongated well-distended villi from base to tip in the absence of total villous atrophy. Villous height and architecture were graded as no blunting of villi, partial/subtotal blunting, or total blunting of villi. The amount of shortening was variable in different biopsies and was graded as: 3:1 to 5:1- Normal/No villous atrophy, 2:1- Partial villous atrophy and 1:1 to 0:1- Total villous atrophy.
The presence of crypt hyperplasia was defined as an increase in the length of crypts or an increase in the number of mitosis due to the expansion of the proliferative compartment from the crypt base, along the length of the crypt. IELs were counted starting from the tip of the villous down along the length of the villous on both sides. Normal IEL count was taken to 20-25/100 enterocytes. 26-29 was taken borderline increased and IELs > 30 was diagnosed as intraepithelial lymphocytosis. The evaluation of these parameters was done based on Modified Marsh Criteria for Celiac disease wherever clinically indicated3 (Table 1).
Table 1.
Modified Marsh-Oberhuber classification
|
Marsh Class
|
Lesion Type
|
Villous atrophy
|
Crypt Hyperplasia
|
IELs
|
| 1 |
Infiltrative |
Absent |
Absent |
Raised |
| 2 |
Infiltrative –hyperplastic |
Absent |
Present |
Raised |
| 3A |
Flat destructive |
Mild |
Present |
Raised |
| 3B |
Flat destructive |
Moderate |
Present |
Raised |
| 3C |
Flat destructive |
Total |
Present |
Raised |
| 4 |
Atrophic hypoplastic |
Total |
Present |
Raised |
Statistical Analysis
Data was collected using preformed data collection forms and case record forms. Data entry was done in Microsoft Excel and analysis using Statistical Package for Social Sciences (SPSS) software version 20/Epi Info/Primer/Win-pepi. Categorical variables were expressed in terms of frequency and percentage, and continuous variables in terms of mean and SD. T test was used to analyze continuous data in order to compare the means of two independent groups. Chi-square test was used to determine the relationship between two categorical variables. Using these tests, P value was obtained. P value less than 0.05 was considered as statistically significant.
Results
A total of 160 cases of suspected malabsorption were included in the study and endoscopic and histopathological examination was done. The number of males and females was 79 (49.4%) and 81 (50.6%) respectively. The most common age of presentation was in the 6th decade of life. The mean age of presentation was 39.4 ± 13.9 years. Most of the small intestinal studied biopsies were from duodenum (84.4%, n=135), followed by ileum (15%, n=24) and jejunum (0.01%, n=1) from jejunum. The most common clinical presentation accompanying chronic diarrhea was abdominal pain (43.8%, n = 70), followed by generalized weakness in 12.9% (n = 26), weight loss in 9% (n = 18), and constipation in 2.5% (n = 5) of cases. Endoscopic findings in the majority of the cases were within normal limits (49.7%, n = 82), followed by duodenitis in 17.6% (n = 29) and scalloped/serrated or fissured duodenal folds in 14.5% (n = 24) of cases (Table 2) The histopathological findings revealed partial villous atrophy in 18.6% (n = 30) and total villous atrophy in 4.4% (n = 7) of patients. Crypt hyperplasia was present in 6.3% (n = 10) and increased IEL count was present in 16.9% (n = 27) of patients. Out of a total of 160 cases of small intestinal studied biopsies, most common histopathological diagnosis was chronic duodenitis (64.4%, n = 103). Celiac disease was diagnosed in 3.1% (n = 5) of cases and only 1.2% (n = 2) of cases were diagnosed as tropical sprue. Specific duodenitis including H. pylori-associated peptic duodenitis and cytomegalovirus (CMV) duodenitis was found in 4 and 1 cases respectively (Table 3).
Table 2.
Endoscopic findings in cases of malabsorption
|
Endoscopicfindings
|
Frequency(n)
|
Percent
|
| Normal mucosal study/no significant finding |
82 |
49.7 |
| Scalloping/serrated/fissured duodenal folds |
24 |
14.5 |
| Reduced duodenal folds |
2 |
1.2 |
| Atrophy of duodenal folds |
11 |
6.7 |
| Whitish mucosa/lymphangiectasia of duodenum |
11 |
6.7 |
| Duodenitis (erosions/erythema/healed mucosa) |
29 |
17.6 |
| Ulcers in ileum |
1 |
0.6 |
| Erythema in ileum |
3 |
1.8 |
| Nodularity in ileum |
2 |
1.2 |
| Stricture in ileum |
0 |
0 |
| Total (multiple answers) |
165 |
100 |
Table 3.
Histopathological diagnosis in cases of malabsorption
|
Histopathologicaldiagnosis
|
Frequency (n)
|
Percent
|
| No pathology |
4 |
2.5 |
| Gastritis |
1 |
0.6 |
| Acute duodenitis |
0 |
0 |
| Chronic duodenitis |
103 |
64.4 |
| Acute on chronic duodenitis |
14 |
8.7 |
| Specific duodenitis |
5 |
3.1 |
| Celiac disease |
5 |
3.1 |
| Tropical sprue |
2 |
1.2 |
| Acute ileitis |
1 |
0.6 |
| Chronic ileitis |
19 |
11.9 |
| Acute on chronic ileitis |
2 |
1.2 |
| Jejunitis |
1 |
0.6 |
| Neuroendocrine hyperplasia |
1 |
0.6 |
| Granulomatous pathology |
1 |
0.6 |
| Brunners gland hyperplasia |
1 |
0.6 |
| Total |
160 |
100 |
Correlation between endoscopic and histopathological findings of all cases of suspected malabsorption was assessed (Table 4). A statistically significant correlation was found between villous atrophy and increased IEL count and also between villous atrophy and crypt hyperplasia (P value < 0.0001). Both normal and abnormal endoscopic mucosal findings had chronic duodenitis as the most common histopathology. In addition, normal endoscopic findings in the duodenum were also seen in celiac disease, tropical sprue, specific duodenitis, and Brunner’s gland hyperplasia. Normal ileal endoscopic findings revealed the most common histopathologic finding as chronic ileitis followed by acute and acute on chronic ileitis and granulomatous inflammation. Most cases of chronic duodenitis 59.8% (n = 49) had a normal mucosal study on endoscopy, 19 cases showed findings of duodenitis including erosions or erythema,15 cases had scalloped, serrated, or fissured duodenal folds (Figure 1). Among total 5 cases of celiac disease 2 cases had normal mucosal study, 2 cases showed significant scalloping of duodenal folds and 1 case showed whitish granular mucosa. Two cases of tropical sprue showed normal mucosal study (Figure 2).
Table 4.
Histopathological diagnosis and its association with endoscopic findings
|
Histopath diagnosis
|
Normalstudy
|
Scallopedduodenalfolds
|
Reducedduodenalfolds
|
Atrophicduodenalfolds
|
Whitish mucosa
|
Duodenitis
|
Ulcers inileum
|
Erythema in ileum
|
Nodularity in ileum
|
| No pathology |
2 (2.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
2 (7.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Gastritis |
1 (1.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Chronic duodenitis |
49 (59.8%) |
15 (62.5%) |
2 (100.0%) |
8 (88.9%) |
10 (90.9) |
19 (70.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Acute on chronic duodenitis |
6 (7.3%) |
3 (12.5 |
0 (0.0%) |
1 (11.1%) |
0 (0.0%) |
4 (14.8%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Specific duodenitis |
3 (3.7%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
2 (7.4) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Celiac disease |
2 (2.4%) |
2 (8.3%) |
0 (0.0%) |
0 (0.0%) |
1 (9.1%) |
0 (0.0) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Tropical sprue |
2 (2.4% |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Acute ileitis |
1 (1.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Chronic ileitis |
11 (13.4%) |
3 (12.5%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
1 (100.0%) |
3 (100.0%) |
1 (100.0%) |
| Acute on chronic ileitis |
2 (2.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Jejunitis |
1 (1.2% |
0 (0.0% |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Neuroendocrine hyperplasia |
0 (0.0%) |
1 (4.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Granulomatous pathology |
1 (1.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Brunners gland hyperplasia |
1 (1.2%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
| Total |
82 (100.0%) |
24 (100.0%) |
2 (100.0%) |
9 (100.0%) |
11 (100.0%) |
27 (100.0%) |
1 (100.0%) |
3 (100.0%) |
1 (100.0%) |
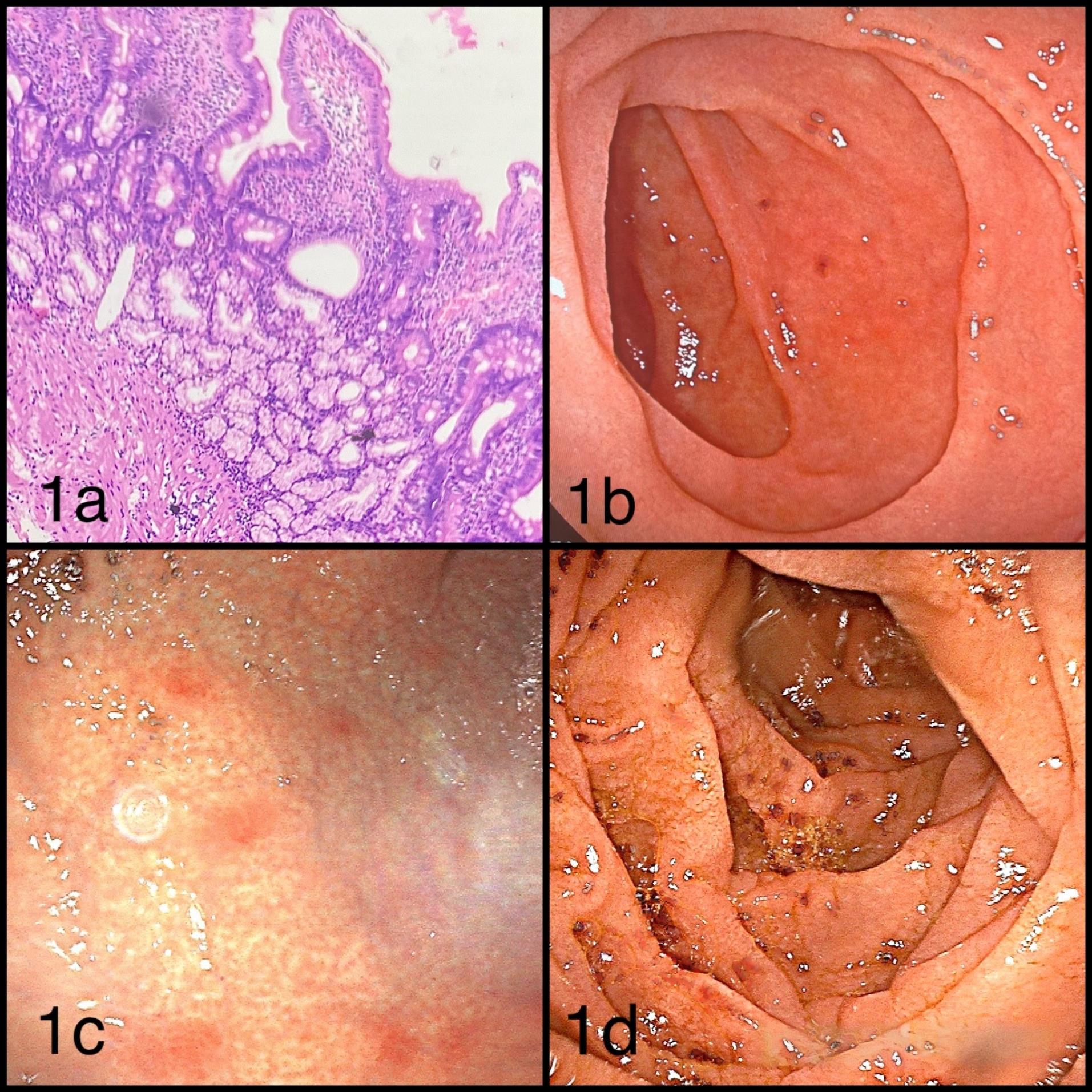
Figure 1.
Histopathology and variety of endoscopy in chronic duodenitis. a: Photomicrohgraph showing mixed inflammatory infiltrate in lamina propria with normal villi:crypt ratio suggestive of Chronic Duodenitis (H&E × 100); b: Normal mucosal study on endoscopy; c: Patchy erythematous mucosa/erythema on endoscopy; d: Scalloped duodenal folds on endoscopy.
.
Histopathology and variety of endoscopy in chronic duodenitis. a: Photomicrohgraph showing mixed inflammatory infiltrate in lamina propria with normal villi:crypt ratio suggestive of Chronic Duodenitis (H&E × 100); b: Normal mucosal study on endoscopy; c: Patchy erythematous mucosa/erythema on endoscopy; d: Scalloped duodenal folds on endoscopy.
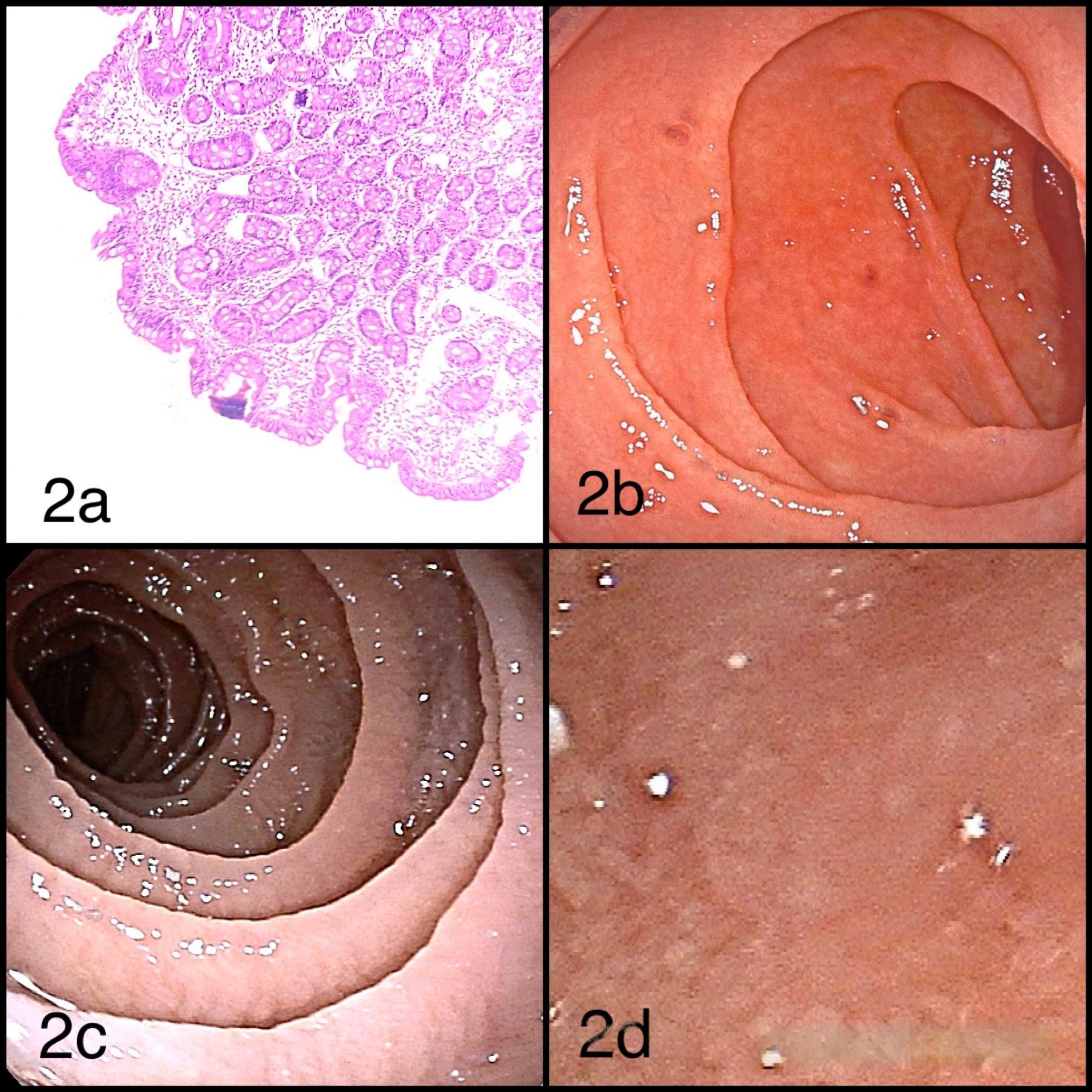
Figure 2.
Histopathology and variety of endoscopy in celiac disease. (a) Photomicrograph showing total villous atrophy with crypt hyperplasia and increased IEL count (H&EX100); (b) Normal mucosal study on endoscopy; (c) Scalloping of duodenal folds on endoscopy; (d) Whitish granular mucosa on endoscopy.
.
Histopathology and variety of endoscopy in celiac disease. (a) Photomicrograph showing total villous atrophy with crypt hyperplasia and increased IEL count (H&EX100); (b) Normal mucosal study on endoscopy; (c) Scalloping of duodenal folds on endoscopy; (d) Whitish granular mucosa on endoscopy.
Discussion
Malabsorption is typically suspected based on the patient’s history, symptoms, and results of standard laboratory tests. Procedures like endoscopy with small intestinal biopsy are frequently necessary to identify the etiology of malabsorption.4 Small intestinal biopsies form the mainstay for making the final diagnosis in suspected cases of malabsorption syndrome.8,9 Due to the wide spectrum of etiologies of malabsorption syndrome, formulating a correct diagnosis requires a thorough correlation of endoscopic and histopathological findings. Such a correlation has been demonstrated in the present study and a comparative analysis of these parameters with various similar studies in literature has been done.
In the present study, the mean age of participants was 39.4 ± 13.9 years ranging from 2 to 60 years and the most common decade of presentation was in the 6th decade in 25.6% of patients. The mean age of presentation was similar with Enache and colleagues’ study, which was 39 ± 11 years.5 Not much difference was observed between our study and Licata and colleagues’ in terms of age with a mean age of 40 ± 16 years.10 The differences in age of disease onset due to a wide range of environmental, genetic, dietary factors, and immunological factors including HLA haplotypes, time of gluten introduction in the diet, the concentration of gluten in the diet, and individual sensitivities to dietary components.11
In our study almost equal sex-wise distribution was found with a male:female ratio of 0.97:1. This was comparable to a study by Meena et al. where almost equal number of males and females were found with a male: female ratio of 1.1:1.12 However in studies by Licata et al and Caio et al a strong female preponderance was present with a male:female ratio of 0.2:1.10,13 A higher preponderance in females has been attributed to physiological and hormonal differences. Apart from chronic diarrhea, pain in abdomen was the most common clinical presentation in 43.8% of cases. Other common complaints were generalized weakness in 12.9% followed by weight loss in 9% and constipation in 2.5% of cases. A similar pattern of presenting complaints was observed in the study by Emami et al in which pain in abdomen was the most common presenting feature followed by chronic diarrhea.14 A considerable number of cases of other symptoms like fatigue/weakness, steatorrhea, flatulence, and constipation were also present in their study. Chronic diarrhea was the most common typical symptom and anemia was the most common atypical symptom in a study by Mansour et al.15 Hence, a wide range spectrum of presenting complaints should be considered for diagnosing important malabsorptive diseases like celiac disease.14
Endoscopic findings in the majority of the cases (49.69%) showed normal mucosal study. Duodenitis which is a broad term used for erosions, erythema, or healed mucosa of duodenum was found to be the second most common finding in 17.57% of patients. This was followed by scalloped, serrated, or fissured duodenal folds in 14.54% of cases. When compared to other similar studies in literature, Pipaliya et al revealed scalloping of duodenal folds to be the most common endoscopic finding in 70% of the patients out of which 68% were later diagnosed to be of tropical sprue and 2% of parasitic infections.16
Histopathological findings revealed partial villous atrophy in 18.6% and total villous atrophy in 4.3% of patients. Crypt hyperplasia was present in 6.25% and increased IEL count was present in 16.9% of patients. Balasubramanian et al showed a similar pattern of morphological abnormalities with the finding of villous atrophy in 23 patients, crypt hyperplasia in 16 patients and raised IEL count/100 enterocytes in 54 patients.17 Devi et al evaluated total of 106 patients and found villous atrophy in 29, crypt hyperplasia in 14 and raised IELs in 15 patients.14 Pipaliya et al found villous atrophy in 51 patients, crypt hyperplasia in 10 patients, and raised IELs in 98 patients.16 In our study, a statistically significant correlation was found between villous atrophy and increased IEL count and also between villous atrophy and crypt hyperplasia (P value < 0.0001). A similar association was found in a study by Karegar et al.1
Malabsorption syndromes can occur due to a wide spectrum of underlying etiologies. In this study, the most common histopathological manifestation was chronic duodenitis of non-specific type in 64.4% of cases. These results were similar to a study by Balasubramanian et al and Devi et al. in which the most common diagnosis was non-specific duodenitis in 40.6% and 45.2% of cases respectively.17,18 The presence of normal villous architecture, absence of crypt hyperplasia, and normal IEL count with mixed inflammation in the lamina propria comprising lymphocytes, plasma cells, and eosinophils were the primary findings in the diagnosis of chronic duodenitis. This suggests that malabsorptive syndromes may not always have a specific underlying cause, except chronic inflammation. Williams et al’s study, also found that 96% of patients had merely an increase in lamina propria inflammation and no clear cause.19 In the study conducted by Mahadeva et al, 82% of the samples revealed non-specific histopathological results.20 When correlated with endoscopic findings, most cases of chronic duodenitis, 47.5% showed normal mucosal study on endoscopy,18% showed findings of duodenitis including erosions or erythema and 14.5% of cases had scalloped, serrated or fissured duodenal folds. Karegar et al. and Challet et al also demonstrated normal mucosal study as the most common endoscopic finding in 58% and 66% of patients respectively.1,21 These variable findings on endoscopy suggest the importance of histopathological diagnosis when no specific clues of underlying etiology are found on upper gastrointestinal endoscopy.
We found 5 cases of celiac disease in this study which were diagnosed based on histopathological findings of total/subtotal partial villous atrophy, crypt hyperplasia, and raised IEL count of > 30 lymphocytes/100 epithelial cells and also positive serology for celiac disease. When classified according to the Modified Marsh Oberhuber classification, all 5 cases fell in the Modified Marsh type 3 category which is defined as the spectrum of changes seen in symptomatic celiac disease. These results were consistent with a study by Meena et al. in which the maximum number of cases were in the Marsh type 3 category.12 Endoscopic findings among a total of 5 cases of celiac disease showed 2 cases with a normal mucosal study, 2 cases with significant scalloping of duodenal folds, and 1 case with whitish granular mucosa. Another well-documented etiology of malabsorption syndrome is tropical sprue. our study, only 2 cases were diagnosed with tropical sprue. Literature suggests that a very thin line of distinction exists between celiac disease and tropical sprue due to which it mostly remains a diagnosis of exclusion. Some of the findings favoring diagnosis of tropical sprue in contrast to celiac sprue, include a higher age of presentation, higher body weight, shorter duration of symptoms, higher hemoglobin levels, lower platelet count, MCV > 91fl, more severe vitamin B12 deficiency, more scalloping of duodenal folds on endoscopy, variable amount of villous atrophy, mononuclear infiltrate in lamina propria, a variable IEL count on histopathology and response to doxycycline and folic acid.16,22 In our study in both cases of tropical sprue, normal mucosal study was found on endoscopy. The diagnosis favored tropical sprue due to the presence of a variable amount of villous atrophy, absence of crypt hyperplasia, and only focally increased IEL count. The changes of tropical sprue in our cases were found in the lower mucosal part which included inflammatory infiltration in the lamina propria with increased eosinophils, however, the upper mucosal region consisting of villi remained normal. As tropical sprue remains a diagnosis of exclusion, final diagnosis should always be supported with negative serology for anti-tissue transglutaminase antibodies as presented in both of our cases. Upper gastrointestinal endoscopy, alone, without histopathological diagnosis could have led to a missed diagnosis of tropical sprue in these cases. These results point out the non-specific nature of upper gastrointestinal endoscopic findings.
Endoscopy has challenges when detecting disorders such as celiac disease, tropical sprue, specific duodenitis, and Brunner’s gland hyperplasia since these diseases frequently include microscopic alterations that cannot be seen with the naked eye.23 Brunner’s gland hyperplasia, which can be manifested as tiny nodules or cysts, may go undetected if they do not dramatically affect the mucosal surface. Furthermore, due to the patchy distribution of these disorders, some duodenal areas may appear normal, resulting in missed diagnosis if biopsies are not taken from affected.23,24 The endoscopic technique and experience of the endoscopist are equally important. Early-stage conditions may manifest with little or localized alterations, whereas subtle abnormalities such as mild erythema can be ignored, especially if the endoscopist is inexperienced.25 High-definition endoscopes and techniques such as chromoendoscopy can improve detection. Insufficient biopsy sampling complicates detection, necessitating a complete diagnostic strategy that includes clinical assessment, serology, and histopathology even when endoscopic findings are normal.26
The duodenal mucosal endoscopy can help to identify certain causes of malabsorption. Crohn’s disease is suggested by aphthae, and primary or secondary lymphangiectasia can be distinguished by small, diffuse, white, punctate lesions. Although similar anomalies may also be present in other disorders, the mosaic-like scalloping of the duodenal folds and the decrease in the number of duodenal folds suggest villous atrophy in celiac disease.27 Balaban et al suggested high specificity of scalloped or fissured duodenal folds for celiac disease.28 However, scalloping is not unique to celiac disease and can also occur in eosinophilic enteritis, giardiasis, amyloidosis, tropical diseases, and enteropathy caused by the human immunodeficiency virus (HIV).27 Numerous fissures or a mosaic-like appearance, where the fissures surround patches of mucosal nodularity, can be additional endoscopic characteristics, or the endoscopic study can sometimes show no mucosal abnormalities at all. The non-specific nature of endoscopic findings has also been supported by Enach et al which suggests a low prevalence of specific endoscopic findings for diagnosing celiac disease.5 A study by Rosa et al suggested that even though they were not diagnostic, the endoscopic signs of villous atrophy have helped in times of suspicion and pointed towards the possibility of a duodenal biopsy for a diagnosis.29 According to these studies, though endoscopic findings may be non-specific in malabsorptive disorders, still it is advisable to go for an endoscopy followed by a biopsy approach as some endoscopic findings can help aid clinical decisions and better management of the patients.5,28 At the same time, our study suggests that, a normal endoscopy or no findings on upper gastrointestinal endoscopy do not rule out the possibility of the existence of malabsorptive disorder. Histopathological evaluation of small intestinal biopsy remains the crucial step for formulating the final diagnosis.
Limitations of the study are that; the ethnicity/demographic details of the cases could not be elaborated, as this was a study carried out at a tertiary care center catering to cosmopolitan culture. Multiple biopsies from different sites were not taken due to the cost constraints.
Study Highlights
What is current knowledge?
-
In cases of malabsorption, endoscopy is performed, and a biopsy is taken when abnormal mucosal findings are observed. The histopathological findings are then correlated with the clinical and endoscopic features to establish the final diagnosis.
What is new here?
-
Endoscopy remains the main diagnostic modality for evaluating malabsorption. However, this study highlights the significance of histopathological findings in cases with normal-appearing mucosa on endoscopy. Therefore, biopsies should be considered even when endoscopic findings appear normal. In addition, in cases of celiac disease, proper correlation among endoscopic, histopathological, and serological findings is essential for accurate diagnosis and precise grading of disease severity.
Conclusion
This study highlights the spectrum of histopathological changes in malabsorption and underscores the importance of its correlation with clinical and endoscopic findings. In the clinical scenario of malabsorption, endoscopy findings vary from normal to abnormal mucosal morphology. Normal mucosal study may also reveal changes in histopathological evaluation. Hence histopathology remains a crucial step for understanding etiopathogenesis thus helping to streamline the management.
Competing Interests
None.
Ethical Approval
Institutional Ethics Committee approval obtained.(Research protocol approval no: IESC/441/2022).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgements
The authors acknowledge the efforts of Dr Veena Joshi, Medical Writer from Central Research Facility, Dr D Y Patil Medical College, Hospital and Research Center, for conducting the statistical analysis and interpretation of the results for the manuscript.
References
- Karegar MM, Kothari K, Mirjolkar AS. Duodenal biopsy in malabsorption: a clinicopathological study. Indian J Pathol Oncol 2016; 3(2):197-201. doi: 10.5958/2394-6792.2016.00039.9 [Crossref] [ Google Scholar]
- Zuvarox T, Goosenberg E, Belletieri C. Malabsorption syndromes. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553106/.
- Villanacci V, Vanoli A, Leoncini G, Arpa G, Salviato T, Bonetti LR. Celiac disease: histology-differential diagnosis-complications A practical approach. Pathologica 2020; 112(3):186-96. doi: 10.32074/1591-951x-157 [Crossref] [ Google Scholar]
- Caio G, Volta U, Sapone A, Leffler DA, De Giorgio R, Catassi C. Celiac disease: a comprehensive current review. BMC Med 2019; 17(1):142. doi: 10.1186/s12916-019-1380-z [Crossref] [ Google Scholar]
- Enache I, Balaban DV, Vasilescu F, Jurcut C, Ionita-Radu F, Popp A. Upper gastrointestinal tract associated lesions in patients with newly diagnosed celiac disease. Gastroenterol Insights 2022; 13(1):77-86. doi: 10.3390/gastroent13010009 [Crossref] [ Google Scholar]
- Leffler DA, Schuppan D. Update on serologic testing in celiac disease. Am J Gastroenterol 2010; 105(12):2520-4. doi: 10.1038/ajg.2010.276 [Crossref] [ Google Scholar]
- Rubio-Tapia A, Hill ID, Semrad C, Kelly CP, Greer KB, Limketkai BN. American College of Gastroenterology guidelines update: diagnosis and management of celiac disease. Am J Gastroenterol 2023; 118(1):59-76. doi: 10.14309/ajg.0000000000002075 [Crossref] [ Google Scholar]
- Arshi J, Huber AR. Celiac Sprue. Pathology Outlines. Available from: https://www.pathologyoutlines.com/topic/smallbowelceliacsprue.html. Accessed September 15, 2023.
- Sleisenger MH, Fordtran JS. Malabsorption and maldigestion. In: Sleisenger MH, Fordtran JS, eds. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia: Saunders/Elsevier; 2010. p. 1741-42.
- Licata A, Cappello M, Arini A, Florena AM, Randazzo C, Butera G. Serology in adults with celiac disease: limited accuracy in patients with mild histological lesions. Intern Emerg Med 2012; 7(4):337-42. doi: 10.1007/s11739-011-0585-8 [Crossref] [ Google Scholar]
- Sleisenger MH, Fordtran JS. Celiac disease and refractory celiac disease. In: Sleisenger MH, Fordtran JS, eds. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia: Saunders/Elsevier; 2010. p. 1799-800.
- Meena DK, Akunuri S, Meena P, Bhramer A, Sharma SD, Gupta R. Tissue transglutaminase antibody and its association with duodenal biopsy in diagnosis of pediatric celiac disease. Pediatr Gastroenterol Hepatol Nutr 2019; 22(4):350-7. doi: 10.5223/pghn.2019.22.4.350 [Crossref] [ Google Scholar]
- Caio G, Volta U, Ursini F, Manfredini R, De Giorgio R. Small bowel adenocarcinoma as a complication of celiac disease: clinical and diagnostic features. BMC Gastroenterol 2019; 19(1):45. doi: 10.1186/s12876-019-0964-6 [Crossref] [ Google Scholar]
- Emami MH, Kouhestani S, Karimi S, Baghaei A, Janghorbani M, Jamali N. Frequency of celiac disease in adult patients with typical or atypical malabsorption symptoms in Isfahan, Iran. Gastroenterol Res Pract 2012; 2012:106965. doi: 10.1155/2012/106965 [Crossref] [ Google Scholar]
- Mansour HH, Mohsen NA, El-Shabrawi MH, Awad SM, Abd El-Kareem D. Serologic, endoscopic and pathologic findings in pediatric celiac disease: a single center experience in a low/middle income country. World J Clin Pediatr 2022; 11(3):295-306. doi: 10.5409/wjcp.v11.i3.295 [Crossref] [ Google Scholar]
- Pipaliya N, Ingle M, Rathi C, Poddar P, Pandav N, Sawant P. Spectrum of chronic small bowel diarrhea with malabsorption in Indian subcontinent: is the trend really changing?. Intest Res 2016; 14(1):75-82. doi: 10.5217/ir.2016.14.1.75 [Crossref] [ Google Scholar]
- Balasubramanian P, Badhe BA, Ganesh RN, Panicker LC, Mohan P. Morphologic spectrum of duodenal biopsies in malabsorption: a study from Southern India. J Clin Diagn Res 2017; 11(7):EC17-21. doi: 10.7860/jcdr/2017/23871.10231 [Crossref] [ Google Scholar]
- Devi CA, Toi PC, Badhe BA, Mohan P, Mandal J. Clinicopathological and microbiological profile of patients with chronic diarrhoea and malabsorption with special emphasis on duodenal biopsies: a study from tertiary care hospital in South India. Int J Med Sci Diagn Res 2022; 6(5):24-33. doi: 10.32553/ijmsdr.v6i5.938 [Crossref] [ Google Scholar]
- Williams L, Dew MJ, Murray LA, Williams DW. Are routine duodenal biopsies taken at the time of an upper GI endoscopy clinically useful?. Gastroenterol Today 2001; 11:73-6. [ Google Scholar]
- Mahadeva S, Wyatt JI, Howdle PD. Is a raised intraepithelial lymphocyte count with normal duodenal villous architecture clinically relevant?. J Clin Pathol 2002; 55(6):424-8. doi: 10.1136/jcp.55.6.424 [Crossref] [ Google Scholar]
- Chellat H, Salihoun M, Kabbaj N, Amrani L, Serraj I, Chaoui Z. Diagnostic Yield of Routine Duodenal Biopsies in Iron Deficiency Anemia for Celiac Disease Diagnosis. Int Sch Res Notices 2013; 2013(1):769519. doi: 10.5402/2013/769519 [Crossref] [ Google Scholar]
- Ghoshal UC, Mehrotra M, Kumar S, Ghoshal U, Krishnani N, Misra A. Spectrum of malabsorption syndrome among adults & factors differentiating celiac disease & tropical malabsorption. Indian J Med Res 2012; 136(3):451-9. [ Google Scholar]
- Stefanolo JP, Zingone F, Gizzi C, Marsilio I, Espinet ML, Smecuol EG. Upper gastrointestinal endoscopic findings in celiac disease at diagnosis: a multicenter international retrospective study. World J Gastroenterol 2022; 28(43):6157-67. doi: 10.3748/wjg.v28.i43.6157 [Crossref] [ Google Scholar]
- Bojanapu S, Mangla V, Mehrotra S, Lalwani S, Mehta N, Nundy S. Brunner’s gland hyperplasia: an unusual duodenal submucosal lesion seen in four patients. J Surg Case Rep 2018; 2018(11):rjy305. doi: 10.1093/jscr/rjy305 [Crossref] [ Google Scholar]
- Januszewicz W, Kaminski MF. Quality indicators in diagnostic upper gastrointestinal endoscopy. Therap Adv Gastroenterol 2020; 13:1756284820916693. doi: 10.1177/1756284820916693 [Crossref] [ Google Scholar]
- Trivedi PJ, Braden B. Indications, stains and techniques in chromoendoscopy. QJM 2013; 106(2):117-31. doi: 10.1093/qjmed/hcs186 [Crossref] [ Google Scholar]
- Sleisenger MH, Fordtran JS. Celiac disease and refractory celiac disease. In: Sleisenger MH, Fordtran JS, eds. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia: Saunders/Elsevier; 2010. p. 1809-10.
- Balaban DV, Popp A, Vasilescu F, Haidautu D, Purcarea RM, Jinga M. Diagnostic yield of endoscopic markers for celiac disease. J Med Life 2015; 8(4):452-7. [ Google Scholar]
- Rosa RM, de Lourdes Abreu Ferrari M, Pedrosa MS, Ribeiro GM, Brasileiro-Filho G, da Cunha AS. Correlation of endoscopic and histological features in adults with suspected celiac disease in a referral center of Minas Gerais, Brazil. Arq Gastroenterol 2014; 51(4):290-6. doi: 10.1590/s0004-28032014000400005 [Crossref] [ Google Scholar]