J Res Clin Med. 13:34675.
doi: 10.34172/jrcm.025.34675
Original Article
Association of hematological, coagulation and biochemical with respiratory insufficiency and mortality in severe COVID-19 patients: A prospective observational study
Mansour Rezaei Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing, 1 
Amir Vahedian-Azimi Conceptualization, Formal analysis, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing, 2
Abbas Samim Formal analysis, Software, Visualization, Writing – review & editing, 3
Nastaran Baghervandi Farkhad Data curation, Investigation, Resources, Writing – review & editing, 1
Afshin Iranpour Data curation, Investigation, Writing – review & editing, 4
Ali Akbar Ghamari Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – review & editing, 1, *
Author information:
1Department of Anesthesiology and Critical Care, Faculty of Medicine, Tabriz University of Medical Science, Tabriz, Iran
2Nursing Care Research Center, Clinical Sciences Institute, Nursing Faculty, Baqiyatallah University of Medical Sciences, Tehran, Iran
3Chemical Injuries Research Center, Systems Biology and Poisonings Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
4Department of Anesthesiology and Critical Care, Al Zahra Hospital, Dubai, UEA
Abstract
Introduction:
Some changes in the peripheral blood and arterial blood gas (ABG) parameters will occur in patients with severe COVID-19 infections. These changes have the potential to provide clues or guidance for the diagnosis, treatment, and prognosis of COVID-19 patients. The aim of this study was to evaluate the association of hemodynamic, peripheral blood markers and arterial blood gas parameters with respiratory insufficiency and mortality rate in severe COVID-19 patients.
Methods:
This single-center, prospective observational study was conducted on severe COVID-19 patients admitted to the general ICU of a university affiliated hospital in the northwest of Iran. Hemodynamic, hematological, coagulation, biochemical and ABG parameters were compared between survivors and non-survivors and also between patients with mild to moderate and severe respiratory insufficiently. Unadjusted and adjusted binary logistic regression analyses were employed to identify risk factors related to the respiratory insufficiency and mortality.
Results:
In adjusted binary logistic regression, low oxygen saturation (odds ratio [OR]: 0.763, 95% CI: 0.037-0.990, P=0.008), elevated polymorphonuclear leukocyte (PMN)/lymphocyte ratio (OR: 1.999, 95% CI: 1.224-3.008, P=0.008), elevated lactate dehydrogenase [LDH] (OR: 1.711, 95% CI: 1.222-2.051, P=0.045), elevated creatine phosphokinase [CPK] (OR: 1.712, 95% CI: 1.323-2.004, P=0.038), high level of [FiO2] (OR: 1.736, 95% CI: 1.419-2.052, P<0.001) and low level of partial pressure of oxygen (PaO2)/FiO2 ratio (OR: 0.894, 95% CI: 0.387-1, P=0.047) had increased risk of ICU mortality.
Conclusion:
The potential risk factors of high LDH, CPK, PMN/lymphocyte ratio, FiO2, low SpO2 and PaO2/FiO2 ratio could help clinicians identify patients at high risk of death early in the ICU admission.
Keywords: Arterial blood gas, Blood coagulation, Coronavirus infections, Intensive care unit, Mortality
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Introduction
The world has been experiencing pandemic caused by SARS-CoV-2 for three years, the virus that causes COVID-19.1-3 To date, COVID-19 has infected over 430 million people and more than 5.9 million deaths worldwide.4 COVID‐19 patients are characterized by pneumonia symptoms, radiographic evidence of pneumonia, respiratory symptoms, and other symptoms such as fever, sore throat, cough, headache, fatigue, anosmia, and diarrhea.5 Symptoms of COVID-19 can vary from person to person and can lead to clinical manifestations of the disease from asymptomatic infection to mild-moderate or severe infection.6 Severe cases are associated with acute respiratory distress syndrome (ARDS), septic shock, metabolic acidosis, coagulation dysfunction, and multiple organ failure, which ultimately results in approximately 54% mortality in these patients.7-10 This condition is life-threatening for patients with severe COVID-19 and requires admission to the intensive care unit (ICU). Therefore, immediate identification of acute respiratory insufficiently and prediction of mortality in severe COVID-19 patients are essential for accurate allocation of health care resources and the possibility of earlier clinical intervention and monitoring to improve clinical outcomes.
Several previous studies found that the hematological, coagulation and arterial blood gas (ABG) parameters were related to the severity and prognosis of patients, and could be used to predict the severity and prognosis of patients with COVID-19.11-17 The relation of certain hematological parameters, including hemoglobin (Hb) and red cell distribution width (RDW), withinCOVID-19 patients has been demonstrated in earlier studies.18,19 A pooled analysis and review study by Henry et al,20 found that the elevated C-reactive protein (CRP), procalcitonin (PCT), and lactate dehydrogenase (LDH) in mild to severe pediatric COVID-19 patients. In a study by Velavan and Meyer, 21 laboratory markers were compared in patients with severe and mild COVID-19 disease and the authors stated that the lymphopenia, ferritin, D-dimer, CRP, cardiac troponin, and LDH were significant parameters with predictive value. A retrospective cohort study by Liu et al,22 demonstrated that CRP and interleukin-6 (IL-6) levels increased in severe stages of the disease, and CRP > 41.8 (mg/L) may be an independent risk factor for progression in the early stage patients with COVID-19. In a retrospective study by Wang,23 revealed that the elevated CRP accompanies lung lesions and therefore reflects the severity of disease.
These findings suggest that some changes in the peripheral blood will occur in patients with SARS-CoV-2 infections. These changes have the potential to provide clues or guidance for the diagnosis, treatment, and prognosis of COVID-19 patients. It is evident from the studies in the literature that various blood parameters are used in determining the severity of COVID-19 infection. However, the parameters that are effective in determining respiratory insufficiently and mortality in severe COVID-19 patients should be clearly revealed. On the other hand, a comprehensive and complete study in this field in the Middle East population with COVID-19 has not been performed to date to measure all these parameters. Therefore, we conducted this study to prospectively analyze the association of hemodynamic, hematological, coagulation, biochemical and ABG parameters with respiratory insufficiency and mortality in severe COVID-19 patients
Methods
Study design
This single-center, prospective observational study was conducted on patients with severe COVID-19, to evaluate the association of hemodynamic, hematological, coagulation, biochemical and arterial blood gas parameters with respiratory insufficiency and mortality rate. The study was conducted in accordance with the Declaration of Helsinki of the World Medical Association.24 The study protocol was reviewed in accordance with the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.25 Written informed consent was obtained from all patients or their legal representatives if they were unable to provide consent
Study population
All patients admitted to the general ICU of Imam Reza Hospital of Tabriz University of Medical Sciences in Tabriz, Iran between January and December, 2021 were included in the study if they met the following inclusion criteria: (a) aged 18 years and over, (b) diagnosed as having severe COVID-19 according to the Guidelines for the Diagnosis and Treatment of Corona Virus Disease,26 to receive this diagnosis patients had one or more of the following: respiratory distress with respiratory rate > 30 breaths/min, oxygen saturation (SpO2) < 93% on room air, or arterial oxygen index (arterial partial pressure of oxygen/fraction of inspired oxygen, PaO2/FiO2) < 300 mm Hg. Laboratory confirmation of COVID-19 which includes positive result on a reverse-transcriptase–polymerase-chain-reaction (RT-PCR) assay of a specimen collected on a nasopharyngeal swab.27 Patients were excluded if an alternative medical diagnosis explained their clinical presentations or had missing outcome and baseline information.
Data collection
Data were collected on (a) demographics (age, gender), (b) comorbidities (diabetes mellitus [DM], hypertension [HTN], hyperlipidemia [HLP] and end-stage renal disease [ESRD]); (c) severity of illness on first day of ICU admission based on Acute Physiology and Chronic Health Evaluation (APACHE) IV and Sequential Organ Failure Assessment (SOFA); (d) respiratory status on first day of admission (conventional O2 therapy, non-invasive mechanical ventilation or invasive mechanical ventilation); (e) respiratory insufficiency that was diagnosed and defined according to the Berlin definition,28 (based on degree of hypoxemia; mild to moderate [100 mm Hg < PaO2/FiO2 ≤ 300 mm Hg] and severe [PaO2/FiO2 ≤ 100 mm Hg] and four ancillary variables for severe cases: radiographic severity, respiratory system compliance [ ≤ 40 mL/cm H2O], positive end-expiratory pressure [ ≥ 10 cm H2O], and corrected expired volume per minute [ ≥ 10 L/min], (f) hemodynamic parameters; pulse rate (PR) beats per minute (BPM), respiratory rate (RR per minute), systolic blood pressure (SBP-mm Hg), diastolic blood pressure (DBP-mm Hg), oxygen saturation (SpO2-%) and body temperature; (g) hematological parameters includes white blood cell (WBC-cells × 109/L), polymorphonuclear leukocyte (PMN) (PMN-%), lymphocytes count (cells × 109/L), PMN/lymphocyte ratio, hemoglobin (Hb-g/dL), and Platelet (Plt- cells × 103/L); (h) coagulation parameters includes partial thromboplastin time (PTT-seconds), international normalized ratio (INR) and D-dimer (ng/mL); (i) biochemical parameters includes blood urea nitrogen (BUN-mg/dL), blood sugar (mg/dL), creatinine (Cr-mg/dL), lactic acid dehydrogenase (LDH-U/L), C-reactive protein (CRP-mg/L), ferritin (μg/L), creatinine phosphokinase (CPK-μg/L), erythrocyte sedimentation rate (ESR-mm/h), aspartate aminotransferase (AST-U/L) and alanine aminotransferase (ALT-U/L), and alkaline phosphatase (ALP- IU/L); (j) ABG parameters includes blood PH, partial pressure of carbon dioxide (PCO2-mm Hg), bicarbonate (HCO3- mEq/L), partial pressure of oxygen (PaO2-mm Hg), fraction of inspired oxygen (FiO2), and PaO2/FiO2 ratio (mm Hg). All the laboratory data including complete blood count (BC-6900, Mindray, Shenzhen, China), serum biochemistry (AU5800, Beckman Coulter, CA, USA), and coagulation tests (ACL TOP 700, Werfen, Barcelona, Spain), were collected from the laboratory information system (LIS). Clinical outcomes including ICU length of stay (LOS), mechanical ventilation (MV), MV duration, and mortality rate were monitored for each patient until deceased or discharged from the ICU.
Statistical analysis
All statistical analysis was done by SPSS software (ver.21) (SPSS Inc. IL, Chicago, USA). The normally distributed of numeric variables was checked by Kolmogorov-Smirnov and Shapiro-Wilk and tests. Normal distributed data were reported as mean and standard deviation (SD) or percentage (%) for continuous and categorical variables, respectively. While non-normal distributed continuous data were reported as median and interquartile range (IQR). To compare the differences in terms of demographic characteristics, clinical data, outcomes, hemodynamic, hematological, coagulation, biochemical and ABG parameters between survivors and non-survivors, and in the patients with different severity of respiratory insufficiency (mild to moderate vs, severe) the Mann-Whitney U test and t-test were used for non-normal distributed and normal distributed continuous variables, respectively, and χ2 test or Fisher’s exact test for categorical variables. Unadjusted and adjusted binary logistic regression models were used to explore the risk factors associated with sufficient respiratory and mortality, associations were reported using the odds ratio (OR) and 95% confidence intervals (CI). In adjusted analysis, according to conditional logistic regression, variables with a P value < 0.05 in the unadjusted analyses were proposed for entry into the model and adjusting was done based on confounding factors including age, gender, comorbidities, severity of illness (APACHE and SOFA scores) and MV. GraphPad Prism 9© (GraphPad Software Inc., La Jolla, CA) was used for forest plot of adjusted binary logistic regression analysis to show the association of parameters with the risk of respiratory sufficiently and mortality. In all analyses, P-values less than 0.05 were considered as significant.
Results
Demographic and clinical characteristics
We enrolled 210 patients with severe COVID-19 including 118 (56.2%) males and 92 (43.8%) females with a mean age of 62.98 ± 16.49 years. According to respiratory insufficiently patients were divided into mild to moderate cases (n = 32, 15.2%) and severe cases (n = 178, 84.8%). There was no significant difference in terms of age (P = 0.135) and gender (P = 0.435) between the two groups. However, the mean of APACHE IV score (P = 0.029) and the median score of SOFA (P = 0.045) was significantly higher in the patients with severe respiratory insufficiently than patients with mild to moderate respiratory insufficiency. More patients with severe respiratory failure underwent MV than patients with mild to moderate respiratory failure (85.4% vs. 68.8%, P = 0.021). Also the mortality rate was significantly higher in the patients with severe respiratory insufficiently than the patients with mild to moderate respiratory insufficiently (72.5% vs. 46.9%, P = 0.004) (Table 1).
Table 1.
Comparison of demographic characteristics and clinical data in patients with different severity of respiratory insufficiency and in survivors and non-survivors groups
|
Variables
|
|
All patients
(n=210)
|
Patients with mild to moderate respiratory insufficiency (n=32)
|
Patients with severe respiratory insufficiency (n=178)
|
P
-value
|
Survivors (n=66)
|
Non-survivors (n=144)
|
P
value
|
| Gender |
Male (%) |
118 (56.2) |
20 (62.5) |
98 (55.1) |
0.435 |
37 (56.1) |
81 (56.3) |
0.980 |
| Female (%) |
92 (43.8) |
12 (37.5) |
80 (44.9) |
|
29 (43.9) |
63 (43.8) |
|
| Age (year) |
Mean ± SD
(Range) |
62.98 ± 16.49
(21-96) |
58.97 ± 21.344
(21-96) |
63.70 ± 15.43
(25-96) |
0.135 |
53.50 ± 16.49
(21-89) |
67.33 ± 14.61
(29-96) |
<0.001*
|
| Comorbidities |
Yes (%) |
155 (73.8) |
22 (68.8) |
133 (74.7) |
0.480 |
41 (62.1) |
114 (79.2) |
0.009*
|
| No (%) |
55 (26.2) |
10 (31.3) |
45 (25.3) |
|
25 (37.9) |
30 (20.8) |
|
Comorbidity
types |
DM (%) |
54 (25.7) |
6 (18.8) |
48 (27) |
0.328 |
16 (24.2) |
38 (26.4) |
0.741 |
| HTN (%) |
77 (36.7) |
13 (40.6) |
64 (36) |
0.614 |
21 (31.8) |
56 (38.9) |
0.324 |
| HLP (%) |
8 (3.8) |
2 (6.3) |
6 (3.4) |
0.433 |
2 (3) |
6 (4.2) |
0.690 |
| ESRD (%) |
4 (1.9) |
0 |
4 (2.2) |
0.398 |
0 |
4 (2.8) |
0.172 |
| Others (%) |
88 (41.9) |
16 (50) |
72 (40.4) |
0.313 |
21 (31.8) |
67 (46.5) |
0.045*
|
| APACHE IV |
Mean ± SD (Range) |
14.88 ± 6.64
(1-36) |
12.53 ± 5.224
(4-24) |
15.30 ± 6.790
(1-36) |
0.029*
|
11.17 ± 5.38
(1-26) |
16.58 ± 6.47
(3-36) |
<0.001*
|
| SOFA |
Median (IQR) |
5 (3-7) |
4 (2-6) |
5 (3-7) |
0.045*
|
3 (1-5) |
6 (4-7) |
<0.001*
|
Respiratory status
on admission |
Mask O2 (%) |
85 (40.5) |
22 (68.8) |
63 (35.4) |
0.002*
|
43 (65.2) |
42 (29.2) |
<0.001*
|
| Non-invasive MV (%) |
27 (12.9) |
2 (6.3) |
25 (14) |
|
14 (21.2) |
13 (9) |
|
| Invasive MV (%) |
98 (46.7) |
8 (25) |
90 (50.6) |
|
9 (13.6) |
86 (61.8) |
|
| ICU LOS |
Median (IQR) |
8 (5-13) |
7 (4-10) |
8 (5-13) |
0.351 |
8.5 (6-12) |
8 (4-13) |
0.507 |
| MV |
Yes (%) |
174 (82.9) |
22 (68.8) |
152 (85.4) |
0.021*
|
31 (47) |
143 (99.3) |
<0.001*
|
| No (%) |
36 (17.1) |
10 (31.3) |
26 (14.6) |
|
35 (53) |
1 (0.7) |
|
| MV duration |
Median (IQR) |
7 (1-11) |
4 (1-8) |
5 (1-10) |
0.115 |
1 (0-7) |
7 (3-11) |
<0.001*
|
| Mortality |
Yes |
144 (68.6) |
15 (46.9) |
129 (72.5) |
0.004*
|
- |
- |
-
|
| No |
66 (31.4) |
17 (53.1) |
49 (27.5) |
|
- |
- |
-
|
Respiratory
insufficiency |
Mild to moderate (%) |
32 (15.2) |
- |
- |
- |
17 (25.8) |
15 (10.4) |
0.004*
|
| Severe (%) |
178 (84.8) |
- |
- |
- |
49 (74.2) |
129 (89.6) |
|
Abbreviations: Diabetes mellitus (DM), Hypertension (HTN), Hyperkeratosis lenticularis perstans (HLP), End-Stage Renal Disease (ESRD), Acute Physiology and Chronic Health Evaluation (APACHE), Sequential Organ Failure Assessment (SOFA), Length of stay (LOS), Mechanical ventilation (MV), * P < 0.05 considered as significant.
Of these 210 severe COVID-19 patients, 66 (31.4%) patients survived, and 144 (68.6%) patients did not survive. A comparison of demographic characteristics and clinical data in the survivors and non-survivors groups is presented in Table 1. Compared with survivors, non-survivors were more likely to be older (67.33 ± 14.61 vs. 53.50 ± 16.49, P < 0.001) and had the comorbidities (79.2% vs. 62.1%, P = 0.009). Non-survivors had higher APACHE IV and SOFA than survivors (P < 0.001). The majority of non-survivors (99.3%) used MV and the MV duration was significantly higher in these patients than the survivors (7 days vs. 1 day, P < 0.001).
Hemodynamic, hematological and coagulation parameters
Comparison of hemodynamic, hematological and coagulation parameters in COVID-19 patients with different severity of respiratory insufficiency and in survivors and non-survivors groups is presented in Table 2. According to the result the SpO2 level was significantly lower in the patients with severe respiratory insufficiently than those with mild to moderate respiratory insufficiently (85.5% vs. 91%, P = 0.005). There were no significant differences in terms of hematological and coagulation parameters between severe group and mild-moderate groups with respiratory failure (P > 0.05). PMN (80.8% vs. 74.7%, P = 0.016), PMN/ lymphocyte ratio (16.5 vs. 10.1, P = 0.001) and INR (1.3 vs. 1.2, P = 0.002), D-dimer (1910 ng/mL vs. 903 ng/mL, P = 0.005) levels in non-survivors were significantly higher than the survivors. However, the levels of SpO2 (78.9% vs. 87.3%, P = 0.001) and lymphocyte (0.87 × 109/L vs. 1.14 × 109/L, P = 0.002) were significantly lower than the survivors.
Table 2.
Comparison of hemodynamic, hematological and coagulation parameters in COVID-19 patients with different severity of respiratory insufficiency and in survivors and non-survivors groups
|
Parameters
|
Normal range
|
Patients with mild to moderate respiratory insufficiency (n=32)
|
Patients with severe respiratory insufficiency (n=178)
|
P
value
|
Survivors
(n=66)
|
Non-survivors (n=144)
|
P
value
|
| Hemodynamic parameters |
| Pulse rate (PR) |
60-100 (BPM) |
95.00 ± 20.13 |
96.22 ± 22.23 |
0.772 |
94.32 ± 18.45 |
96.82 ± 23.30 |
0.443 |
| Respiratory rate (RR) |
12 to 20 (BPM) |
28.5 (22.25-32.75) |
30 (21-31.25) |
0.911 |
29.08 (20-30) |
29.94 (22.25-34.5) |
0.272 |
| Systolic blood pressure (SBP) |
120-130 (mm Hg) |
124.16 ± 18.65 |
123.47 ± 28.15 |
0.895 |
123.03 ± 18.68 |
123.83 ± 29.96 |
0.843 |
| Diastolic blood pressure (DBP) |
< 80 (mm Hg) |
74.5 (70-80.75) |
75 (70-85) |
0.801 |
76.06 (70-80.25) |
77.11 (70-87) |
0.819 |
| Oxygen saturation (SpO2) |
≥ 95% |
91 (84.5-94.75) |
85.5 (70-92) |
0.005*
|
86.73 (83-95.25) |
78.96 (66-91) |
0.001*
|
| Temperature |
36.1°C to 37.2°C |
37 (37-37.1) |
37 (37-37.5) |
0.330 |
36.8 (36.9-37.2) |
37.2 (37-37.5) |
0.176 |
| Hematological parameters |
| White blood cell (WBC) |
4.5–11.0 x 109/L |
8.50 (7.25-11.75) |
9.50 (6.25-13.75) |
0.188 |
10.25 (5.60-12.75) |
11.25 (7.12-13.75) |
0.092 |
| PMN |
40% to 80% |
86 (76-92) |
88 (81-92) |
0.788 |
74.7 (75.1-90.1) |
80.8 (81.9-92.6) |
0.016*
|
| Lymphocyte |
1.0 - 4.8 x 109/L |
0.82 (0.53-1.19) |
0.71 (0.5-1.31) |
0.496 |
1.14 (0.57-1.41) |
0.87 (0.42-1.24) |
0.002*
|
| PMN/lymphocyte ratio |
- |
11.1 (6.7-18.1) |
12.4 (6.3-18.6) |
0.523 |
10.1 (5.1-16.1) |
16.5 (7.1-22.2) |
0.001*
|
| Hemoglobin (Hb) |
M: 13.2 to 16.6 (g/dL)
F: 11.6 to 15 (g/dL) |
12.462 ± 2.351 |
12.814 ± 2.099 |
0.392 |
12.80 ± 2.021 |
12.74 ± 2.194 |
0.858 |
| Platelet (Plt) |
150-450 × 103 per μL |
218.50 ± 73.36 |
204.25 ± 80.23 |
0.353 |
216.91 ± 78.83 |
202.64 ± 80.29 |
0.251 |
| Coagulation parameters |
| Partial thromboplastin time (PTT) |
60-70 seconds |
36 (30-43.75) |
34 (30-42.25) |
0.464 |
40.23 (29.7-41.25) |
42.7 (30-43.75) |
0.477 |
| International normalized ratio (INR) |
0.8–1.2 |
1.2 (1.1-1.3) |
1.1 (1.1-1.3) |
0.953 |
1.2 (1.0-1.2) |
1.3 (1.1-1.3) |
0.002*
|
| D-dimer |
≥ 500 (ng/mL) |
1205 (1014.5-5410.5) |
1398 (539.25-5375) |
0.649 |
913 (300-2435.5) |
1910 (848-7558.5) |
0.005*
|
Polymorphonuclear leukocyte (PMN), * P < 0.05 considered as significant.
Biochemical parameters
Comparison of biochemical parameters in COVID-19 patients with different severity of respiratory insufficiency and in survivors and non-survivors groups is shown in Table 3. There were no significant differences in terms of biochemical parameters in the patients with mild-moderate respiratory insufficiently than those with severe respiratory insufficiently (P > 0.05), except LDH level was significantly higher in the patients with severe respiratory insufficiently than those with mild to moderate respiratory insufficiently (1027 U/L vs. 704 U/L, P = 0.002). According to the results of comparing between survivors and non-survivors groups, BUN (32 vs. 22.5, P < 0.001), blood sugar (168.5 mg/dL vs. 143.5 mg/dL, P = 0.036), Cr (1.26 mg/dL vs. 1.01 mg/dL, P < 0.001), LDH (1092 U/L vs. 788.5 U/L, P < 0.001), CPK (256 μg/L vs. 113.5 μg/L, P < 0.001) and ESR (53.91 mm/h vs. 42.69 mm/h, P = 0.033) were significantly higher in the non-survivors than the survivors.
Table 3.
Comparison of biochemical parameters in COVID-19 patients with different severity of respiratory insufficiency and in survivors and non-survivors groups
|
Parameters
|
Normal range
|
Patients with mild to moderate respiratory insufficiency (n=32)
|
Patients with severe respiratory insufficiency (n=178)
|
P
-value
|
Survivors
(n=66)
|
Non-survivors (n=144)
|
P
-value
|
| Blood urea nitrogen (BUN) |
6 to 24 (mg/dL) |
25 (18-35) |
30 (20.75-45) |
0.091 |
22.5 (15-30.25) |
32 (23-47) |
<0.001*
|
| Blood sugar |
< 140 (mg/dL) |
148 (111.5-274.5) |
160 (121.5-245) |
0.733 |
143.5 (106.5-247.25) |
168.5 (125-244.5) |
0.036*
|
| Creatinine (Cr) |
M: 0.7 to 1.3 (mg/dL)
F: 0.6 to 1.1 (mg/dL) |
1.04 (0.85-1.50) |
1.19 (0.92-1.71) |
0.129 |
1.01 (0.85-1.22) |
1.26 (1-1.94) |
<0.001*
|
| Lactic Acid Dehydrogenase (LDH) |
140 to 280 units per liter (U/L) |
747 (560-1046) |
1027 (728-1401.5) |
0.002*
|
788.5 (556.75-1098.25) |
1092 (816-1472) |
<0.001*
|
| C-Reactive Protein (CRP) |
< 10 (mg/L) |
51 (18-169) |
62.5 (24-119) |
0.902 |
54 (18.12-97.65) |
63 (23.25-128) |
0.531 |
| Ferritin |
M: 24 to 336 (μg/L)
F: 11 to 307 (μg/L) |
618.96 ± 340.33 |
764.13 ± 542.58 |
0.392 |
612 ± 523.60 |
821.9 ± 509.5 |
0.074 |
| Creatinine phosphokinase (CPK) |
10 to 120 (μg/L) |
231 (64-360) |
165.5 (76-375.75) |
0.986 |
113.5 (57-280.5) |
256 (93-523) |
<0.001*
|
| Erythrocyte sedimentation rate (ESR) |
M: 0 to 22 (mm/hr)
F: 0 to 29 (mm/hr) |
46.57 ± 27.42 |
50.84 ± 30.63 |
0.534 |
42.69 ± 24.10 |
53.91 ± 32.16 |
0.033*
|
| Aspartate aminotransferase (AST) |
8 to 33 units per liter (U/L) |
41 (30-59) |
54 (33-83) |
0.055 |
47 (29-71) |
53 (35.25-83) |
0.111 |
| Alanine aminotransferase (ALT) |
4 to 36 units per liter (U/L) |
28.5 (19.5-52.75) |
38.5 (22-59) |
0.102 |
42 (22.75-62.75) |
33 (22-54) |
0.235 |
| Alkaline Phosphatase (ALP) |
44 to 147 (IU/L) |
193.5 (143-275.25) |
200.5 (154.25-275.5) |
0.496 |
191 (149.25-254.25) |
203 (154.75-280.75) |
0.528 |
All data presented in median (IQR), except ferritin and ESR are presented in mean ± SD. * P < 0.05 considered as significant.
ABG parameters
Among the ABG indices, PCO2 (39.75 mm Hg vs. 34.80 mm Hg, P = 0.002) and FiO2 (100% vs. 40%, P < 0.001) were significantly higher in the patients with severe respiratory insufficiently than those with mild-moderate respiratory insufficiently. Meanwhile, PaO2 (41 mm Hg vs. 69.6 mm Hg, P < 0.001) and PaO2/FiO2 ratio (46 vs. 141.30, P < 0.001) were significantly lower in the patients with severe respiratory insufficiently than those with mild-moderate respiratory insufficiently (Table 4). All ABG parameters were significantly differences between survivors and non-survivors; PCO2 (40.4 mm Hg vs. 38.1 mm Hg, P = 0.019) and FiO2 (100% vs. 60%, P < 0.001) were significantly higher in the non-survivors than the survivors. However, blood PH (7.3 vs. 7.4, P < 0.001), HCO3 (21.5 mEq/L vs. 23.7 mEq/L, P = 0.024) and PaO2/FiO2 ratio (46 vs. 68, P < 0.001) were significantly lower in the non-survivors than the survivors (Table 4).
Table 4.
Comparison of arterial blood gas (ABG) parameters in COVID-19 patients with different severity of respiratory insufficiency and in survivors and non-survivors groups
|
Parameters
|
Normal range
|
Patients with mild to moderate respiratory insufficiency (n=32)
|
Patients with severe respiratory insufficiency (n=178)
|
P
value
|
Survivors
(n=66)
|
Non-survivors (n=144)
|
P
value
|
| Blood PH |
7.35 to 7.45 |
7.38 (7.30-7.44) |
7.36 (7.26-7.41) |
0.104 |
7.4 (7.36-7.45) |
7.32 (7.24-7.4) |
<0.001*
|
| Partial pressure of carbon dioxide (PCO2) |
35 to 45 (mm Hg) |
34.80 (28.65-40.85) |
39.75 (34.77-48.70) |
0.002*
|
38.1 (32.8-42.7) |
40.4 (34.7-51.15) |
0.019*
|
| Bicarbonate (HCO3) |
22 to 28 (mEq/L) |
21.25 (17.65-24.52) |
22.15 (18.77-25.50) |
0.343 |
23.7 (19.8-25.7) |
21.5 (18-24.97) |
0.024*
|
| Partial pressure of oxygen (PaO2) |
75 to 100 (mm Hg) |
69.60 (50.42-93.50) |
41 (30.57-57.12) |
<0.001*
|
44.05 (30.1-60.2) |
43.7 (33.9-60) |
0.862 |
| Fraction of inspired oxygen (FiO2) |
21% |
40 (40-60) |
100 (80-100) |
<0.001*
|
60 (40-100) |
100 (100-100) |
<0.001*
|
| PaO2/FiO2 ratio |
- |
141.30 (118.56-179.62) |
46 (35-63) |
<0.001*
|
68 (46-103) |
46 (35-69) |
<0.001*
|
All data presented in median (IQR). * P < 0.05 considered as significant.
Unadjusted and adjusted binary logistic regression findings
In unadjusted binary logistic regression analysis, the odds ratio (OR) of mortality was significantly increased with higher levels of PMN/lymphocyte ratio (OR: 1.078, 95% CI: 1.035-3.123, P < 0.001), D-dimer (OR: 1.701, 95% CI: 1.008-2.876, P = 0.022), BUN (OR: 1.033, 95% CI: 1.013-3.054, P = 0.001), Cr (OR: 2.033, 95% CI: 1.257-3.295, P = 0.004), LDH (OR: 3.001, 95% CI: 1.001-5.002, P = 0.004), CPK (OR: 1.323, 95% CI: 1.001-3.523, P = 0.007), ESR (OR: 1.095, 95% CI: 1.021-3.29, P = 0.035), PCO2 (OR: 1.337, 95% CI: 1.011-3.064, P = 0.006) and FiO2 (OR: 1.438, 95% CI: 1.025-3.051, P < 0.001). However, the OR of mortality was significantly decreased with higher SpO2 (OR: 0.961, 95% CI: 0.438-0.985, P = 0.001), lymphocyte (OR: 0.947, 95% CI: 0.008-0.988, P = 0.012) and PaO2/FiO2 ratio (OR: 0.991, 95% CI: 0.605-0.997, P = 0.003). According to the adjusted analysis, minimal evidence of reduce OR for mortality was obtained from higher levels of SpO2 (OR: 0.763, 95% CI: 0.037-0.990, P = 0.008) and PaO2/FiO2 ratio (OR: 0.894, 95% CI: 0.387-1, P = 0.047). Meanwhile, the risk of mortality was increased with age (OR: 1.838, 95% CI: 1.204-2.062, P = 0.002), comorbidities (OR: 2.493, 95% CI: 1.309-4.604, P = 0.027), higher score of APACHE IV (OR: 1.69, 95% CI: 1.217-2.167, P = 0.015), SOFA score (OR: 1.313, 95% CI: 1.127-2.529, P < 0.001), and higher level of PMN/lymphocyte ratio (OR: 1.999, 95% CI: 1.224-3.008, P = 0.008), LDH (OR: 1.711, 95% CI: 1.222-2.051, P = 0.045), CPK (OR: 1.712, 95% CI: 1.323-2.004, P = 0.038) and FiO2 (OR: 1.736, 95% CI: 1.419-2.052, P < 0.001) (Figure 1).
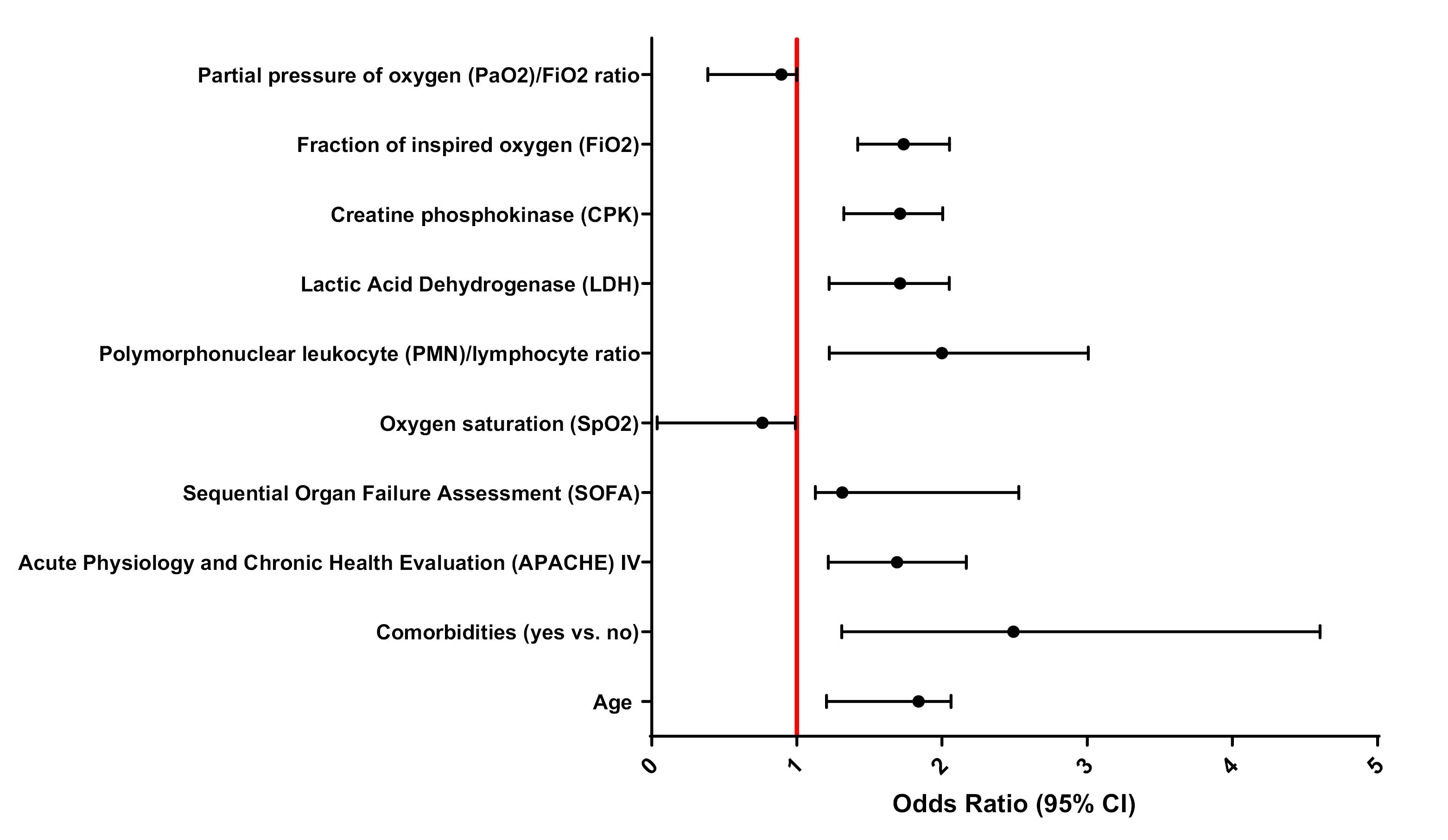
Figure 1.
Forest plot of adjusted binary logistic regression analysis to show the association of parameters with the risk of mortality in patients with COVID-19
.
Forest plot of adjusted binary logistic regression analysis to show the association of parameters with the risk of mortality in patients with COVID-19
In adjusted binary logistic regression, the OR of severe respiratory insufficiently was reduced with higher level of SpO2 (OR: 0.853, 95% CI: 0.517-0.991, P = 0.015), PaO2 (OR: 0.831, 95% CI: 0.608-0.955, P < 0.001) and PaO2/FiO2 ratio (OR: 0.733, 95% CI: 0.411-0.956, P < 0.001). However, the OR of severe respiratory insufficiently was reduced with higher level of LDH (OR: 1.689, 95% CI: 1.344-3.002, P = 0.009) and FiO2 (OR: 1.567, 95% CI: 1.344-3.091, P < 0.001) (Figure 2).
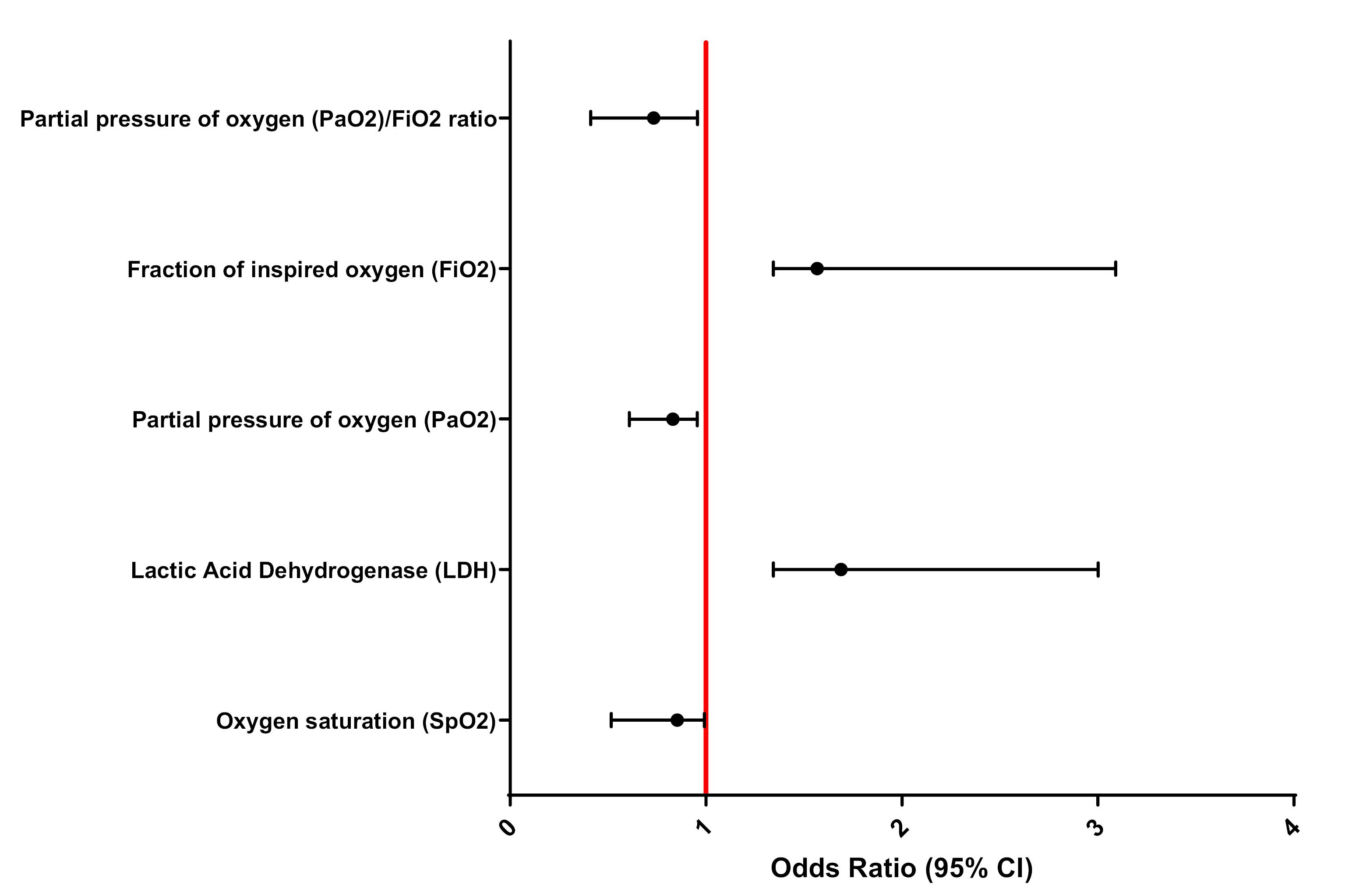
Figure 2.
Forest plot of adjusted binary logistic regression analysis to show the association of parameters with the risk of respiratory insufficiency in patients with COVID-19
.
Forest plot of adjusted binary logistic regression analysis to show the association of parameters with the risk of respiratory insufficiency in patients with COVID-19
Discussion
In this single-center, prospective, observational study, several risk factors for respiratory insufficiently and mortality were identified in ICU patients with severe COVID-19. Consistent with other research, we also found that older age, having comorbidities, and higher severity illness based on APACHE IV and SOFA scores were independently associated with mortality. While none of these factors were not related to respiratory insufficiency in severe COVID-19 patients. Patients with poor blood oxygen saturation (SpO2 ≤ 80), higher inflammation and lower immunity with elevated PMN/lymphocyte ratio (PMN/lymphocyte ratio > 16.5), lung infections with elevated LDH (LDH > 1000 U/L), muscle damage with elevated CPK ( ≥ 250 μg/L), high level of FiO2 (100% after intubation) and severity of hypoxemia with low level of PaO2/FiO2 ratio had increased risk of ICU mortality. In addition, lower blood oxygen saturation (SpO2 ≤ 80), decreased oxygen levels in the inhaled air with low PaO2 (PaO2 < 70 mm Hg), severity of hypoxemia with low level of PaO2/FiO2 ratio, high level of FiO2 and high lung infection with elevated LDH had increased risk of severe respiratory insufficiently in patients with severe COVID-19.
Consistent with previous literature, in adjusted analysis, we observed that elevated LDH and CPK to be associated with mortality in COVID-19 patients. LDH is an intracellular enzyme found in cells in almost all organ systems with highest levels in heart, liver, lungs, muscles, kidneys and blood cells. LDH enzyme involved in energy production that converts lactate into pyruvate due to severe tissue destruction caused by sepsis, malign diseases, and severe infections in many tissues. LDH is a general indicator of an acute or chronic tissue damage and is considered an inflammatory marker.29 LDH has been described to be increased during acute and severe lung damage, and elevated LDH values has been found in other interstitial lung infections.30,31 In CoVID-19 patients, LDH and CRP might represent an expression of lung damage and might reflect the respiratory distress consequent to the abnormal inflammation status. A pooled analysis study by Henry et al,32 on 9 published studies showed that the elevated LDH levels were associated with approximately 6-fold increase in odds of developing severe disease and a 16-fold increase in odds of mortality in patients with COVID-19. In a study by Wu et al,33 on 87 cases confirmed by COVID-19 infection, significant differences in LDH levels were found between non-severe and severe group. The authors stated that LDH level was an indicator for pneumonia caused by COVID-19, which increases with severe pneumonia and decreases when pneumonia was resolved.33 CPK is a marker of muscle damage; when a muscle is damaged, CPK leaks into the bloodstream. It has also been found to increase in patients who have died and those with severe illnesses.34,35 A systematic review and meta-analysis study by Akbar et al,36 on 14 studies showed that the elevated CPK levels were associated with increased mortality and severity in patients with COVID-19. SARS-CoV-2 uses the angiotensin converting enzyme 2 (ACE2) receptor to invade human airway cells and cause infection. Due to its presence in various tissues, the virus can directly invade skeletal muscle and the nervous system via the same pathway. Immune pathways may also help cause muscle damage in patients with COVID-19. In addition, dehydration and hypovolemia in patients with COVID-19 may contribute to renal dysfunction and subsequent elevated CPK levels.35,37
The PMN/lymphocyte ratio in peripheral blood reflects the balance between systemic inflammation (as indicated by the PMN count include neutrophils, eosinophils, basophils, and mast cells) and adaptive immunity (lymphocyte count) and is emerging as a prognostic biomarker in many diseases.38-41 In the current study, we observed the significantly lower level of lymphocytes (lymphopenia) and higher level of PMN in non-survivor patients than the survivors. An increase in PMN/lymphocyte ratio is determined by an increase of PMN and/or reduction in lymphocytes. High levels of PMN/lymphocyte ratio in the blood are most often caused by infections that showed high inflammation and low immunity. In addition, higher PMN/lymphocyte ratio was associated with increased ICU mortality. A cohort study by Liu et al,42 on 245 COVID-19 patients showed that the 8% higher risk of in-hospital mortality for each unit increases in higher neutrophil to lymphocyte ratio (NLR). According to evidence, cytokine storm induced by virus invasion is a phenomenon of an excessive inflammatory reaction that rapidly produces many cytokines, especially IL-6, in response to microbial infection.43 This phenomenon is considered an important contributor to COVID-19. Persistent stimulation by the virus may lead to a reduction in lymphocytes and increase in PMN.44-46 Similarly, many previous studies showed lymphopenia in patients with COVID-19.47,48
Early identification and adequate treatment of COVID-19 patients at high risk for acute respiratory failure and mortality is very important. Today, chest CT scan plays a key role in diagnosing and assessing the severity of lung involvement in COVID-19 pneumonia,49 but unfortunately CT scans are not always available in addition to the high cost. Several limitations need to be acknowledged. Firstly, the sample size is relatively small, though we collected all confirmed patients with COVID-19 admitted to the general ICU in single-center according to convenience sampling. Secondly, some laboratory tests (for example ferritin, ESR and D-dimer) were not performed on all patients; missing data might lead to bias in clinical characteristics between groups. Thirdly, our study participants only included severe cases of COVID-19, leading to limited generalizability to cases with mild symptoms. Fourthly, several potential confounders including health-related behaviors and the detailed treatment history for COVID-19 before admission, which has a significant impact on adverse clinical events, were not available to collect. Our study has limitations i.e. not multicenter study and small sample size.
Study Highlights
What is current knowledge?
-
Hematological, coagulation, and biochemical parameter alterations are well-documented in COVID-19 and correlate with disease severity.
-
Elevated inflammatory markers (CRP, D-dimer, LDH) and lymphopenia are established prognostic indicators.
-
ABG parameters, particularly PaO₂/FiO₂ ratio, are crucial for assessing respiratory failure in critical COVID-19 cases.
-
Age, comorbidities, and illness severity scores remain consistent mortality predictors in ICU settings.
What is new here?
-
This prospective study provides comprehensive multi-parameter analysis in Middle-Eastern severe COVID-19 patients, addressing regional literature gaps.
-
We identify PMN/lymphocyte ratio, CPK, and LDH as independent mortality predictors in confounder-adjusted models.
-
LDH demonstrates significant association with respiratory insufficiency severity, offering valuable stratification utility.
-
The study establishes a novel combination of accessible parameters for early detection of high-risk patients, enabling timely intervention in ICU settings.
Conclusion
A better understanding of the clinical characteristics of patients with severe COVID19 in the early stages of hospitalization is timely for patients at risk of poor outcome, as laboratory data from the onset of the disease to admission are often not clinically available. The predictive value of dynamic changes in LDH, CPK, PMN/lymphocyte ratios, FiO2, SpO2, and PaO2/ FiO2 ratios contribute to early detection of COVID patients at high risk of death in the ICU and provide early supportive. These findings may assist physicians in early triage of patients with severe COVID-19 with a high risk of mortality.
Competing Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The protocol study was reviewed and approved by the Research Council of Tabriz University of Medical Sciences under ethics code (IR.TBZMED.REC.1399.772), in accordance with the Declaration of Helsinki of the World Medical Association. In addition, this study was conducted based on recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 25 Written informed consent was obtained from all patients or their legal representatives if they were unable to provide consent.
Acknowledgements
The authors would like to thank to the Vice Chancellor for Research and Development of Tabriz University of Medical Sciences and Clinical Research Development Unit, Taleghani Hospital, Tabriz University of Medical Sciences, Tabriz, Iran for kind supports.
The authors would like to thank Clinical Research Development Unit, Taleghani Hospital, Tabriz University of Medical Sciences, Tabriz, Iran for kind supports. The authors thank the “Clinical Research Development Unit of Baqiyatallah Hospital” for their guidance and advice.
References
- Krishnan A, Hamilton JP, Alqahtani SA, Woreta TA. COVID-19: an overview and a clinical update. World J Clin Cases 2021; 9(1):8-23. doi: 10.12998/wjcc.v9.i1.8 [Crossref] [ Google Scholar]
- Chittora D, Meena BR, Mittholiya S, Sharma K. Updates of COVID-19. Res Biomed Eng 2021; 37(4):835-48. doi: 10.1007/s42600-021-00140-9 [Crossref] [ Google Scholar]
- Mahmoodpoor A, Shadvar K, Ghamari AA, Mohammadzadeh Lameh M, Asghari Ardebili R, Hamidi M. Management of critically ill patients with COVID-19: what we learned and what we do. Anesth Pain Med 2020; 10(3):e104900. doi: 10.5812/aapm.104900 [Crossref] [ Google Scholar]
- Our World in Data. COVID-19 Data Explorer. 2022. Available from: https://ourworldindata.org/explorers/coronavirus-data-explorer.
- Baj J, Karakuła-Juchnowicz H, Teresiński G, Buszewicz G, Ciesielka M, Sitarz R. COVID-19: specific and non-specific clinical manifestations and symptoms: the current state of knowledge. J Clin Med 2020; 9(6):1753. doi: 10.3390/jcm9061753 [Crossref] [ Google Scholar]
- Struyf T, Deeks JJ, Dinnes J, Takwoingi Y, Davenport C, Leeflang MM. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19. Cochrane Database Syst Rev 2021; 2(2):CD013665. doi: 10.1002/14651858.CD013665.pub2 [Crossref] [ Google Scholar]
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020; 395(10223):507-13. doi: 10.1016/s0140-6736(20)30211-7 [Crossref] [ Google Scholar]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395(10223):497-506. doi: 10.1016/s0140-6736(20)30183-5 [Crossref] [ Google Scholar]
- Mahendra M, Nuchin A, Kumar R, Shreedhar S, Mahesh PA. Predictors of mortality in patients with severe COVID-19 pneumonia - a retrospective study. Adv Respir Med 2021; 89(2):135-44. doi: 10.5603/ARM.a2021.0036 [Crossref] [ Google Scholar]
- Hamishehkar H, Beigmohammadi MT, Abdollahi M, Ahmadi A, Mahmoodpour A, Mirjalili MR. Identification of enhanced cytokine generation following sepsis Dream of magic bullet for mortality prediction and therapeutic evaluation. Daru 2010; 18(3):155-62. [ Google Scholar]
- Nigam JS, Kumar A, Sinha R, Haripriya H, Kumar N, Surabhi Surabhi. Association of peripheral blood parameters with outcomes of COVID-19 infection in a tertiary care setting of eastern India: an institute-based study. Cureus 2021; 13(12):e20745. doi: 10.7759/cureus.20745 [Crossref] [ Google Scholar]
- Ertekin B, Yortanlı M, Özelbaykal O, Doğru A, Girişgin AS, Acar T. The relationship between routine blood parameters and the prognosis of COVID-19 patients in the emergency department. Emerg Med Int 2021; 2021:7489675. doi: 10.1155/2021/7489675 [Crossref] [ Google Scholar]
- Szklanna PB, Altaie H, Comer SP, Cullivan S, Kelliher S, Weiss L. Routine hematological parameters may be predictors of COVID-19 severity. Front Med (Lausanne) 2021; 8:682843. doi: 10.3389/fmed.2021.682843 [Crossref] [ Google Scholar]
- Turcato G, Panebianco L, Zaboli A, Scheurer C, Ausserhofer D, Wieser A. Correlation between arterial blood gas and CT volumetry in patients with SARS-CoV-2 in the emergency department. Int J Infect Dis 2020; 97:233-5. doi: 10.1016/j.ijid.2020.06.033 [Crossref] [ Google Scholar]
- Sayad B, Rahimi Z. Blood coagulation parameters in patients with severe COVID-19 from Kermanshah province, Islamic Republic of Iran. East Mediterr Health J 2020; 26(9):999-1004. doi: 10.26719/emhj.20.105 [Crossref] [ Google Scholar]
- Huang D, Yang H, Yu H, Wang T, Chen Z, Yao R. Diagnostic value of hematological and biochemical parameters combinations for predicting coronavirus disease 2019 (COVID-19) in suspected patients. Am J Med Sci 2021; 362(4):387-95. doi: 10.1016/j.amjms.2021.04.006 [Crossref] [ Google Scholar]
- Bilgir F, Çalık Ş, Demir İ, Bilgir O. Roles of certain biochemical and hematological parameters in predicting mortality and ICU admission in COVID-19 patients. Rev Assoc Med Bras (1992) 2021; 67(Suppl 1):67-73. doi: 10.1590/1806-9282.67.Suppl1.20200788 [Crossref] [ Google Scholar]
- Pan Y, Ye G, Zeng X, Liu G, Zeng X, Jiang X. Can routine laboratory tests discriminate SARS-CoV-2-infected pneumonia from other causes of community-acquired pneumonia?. Clin Transl Med 2020; 10(1):161-8. doi: 10.1002/ctm2.23 [Crossref] [ Google Scholar]
- Wang C, Deng R, Gou L, Fu Z, Zhang X, Shao F. Preliminary study to identify severe from moderate cases of COVID-19 using combined hematology parameters. Ann Transl Med 2020; 8(9):593. doi: 10.21037/atm-20-3391 [Crossref] [ Google Scholar]
- Henry BM, Benoit SW, de Oliveira MH, Hsieh WC, Benoit J, Ballout RA. Laboratory abnormalities in children with mild and severe coronavirus disease 2019 (COVID-19): a pooled analysis and review. Clin Biochem 2020; 81:1-8. doi: 10.1016/j.clinbiochem.2020.05.012 [Crossref] [ Google Scholar]
- Velavan TP, Meyer CG. Mild versus severe COVID-19: laboratory markers. Int J Infect Dis 2020; 95:304-7. doi: 10.1016/j.ijid.2020.04.061 [Crossref] [ Google Scholar]
- Liu F, Li L, Xu M, Wu J, Luo D, Zhu Y. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J Clin Virol 2020; 127:104370. doi: 10.1016/j.jcv.2020.104370 [Crossref] [ Google Scholar]
- Wang L. C-reactive protein levels in the early stage of COVID-19. Med Mal Infect 2020; 50(4):332-4. doi: 10.1016/j.medmal.2020.03.007 [Crossref] [ Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 2013; 310(20):2191-4. doi: 10.1001/jama.2013.281053 [Crossref] [ Google Scholar]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 2008; 61(4):344-9. doi: 10.1016/j.jclinepi.2007.11.008 [Crossref] [ Google Scholar]
- Xu Y, Chen Y, Tang X. Guidelines for the diagnosis and treatment of coronavirus disease 2019 (COVID-19) in China. Glob Health Med 2020; 2(2):66-72. doi: 10.35772/ghm.2020.01015 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease is Suspected: Interim Guidance, 13 March 2020. WHO; 2020. Available from: https://apps.who.int/iris/handle/10665/331446.
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E. Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012; 307(23):2526-33. doi: 10.1001/jama.2012.5669 [Crossref] [ Google Scholar]
- Wu Y, Lu C, Pan N, Zhang M, An Y, Xu M. Serum lactate dehydrogenase activities as systems biomarkers for 48 types of human diseases. Sci Rep 2021; 11(1):12997. doi: 10.1038/s41598-021-92430-6 [Crossref] [ Google Scholar]
- Bartziokas K, Kostikas K. Lactate dehydrogenase, COVID-19 and mortality. Med Clin (Barc) 2021; 156(1):37. doi: 10.1016/j.medcli.2020.07.043 [Crossref] [ Google Scholar]
- Poggiali E, Zaino D, Immovilli P, Rovero L, Losi G, Dacrema A. Lactate dehydrogenase and C-reactive protein as predictors of respiratory failure in CoVID-19 patients. Clin Chim Acta 2020; 509:135-8. doi: 10.1016/j.cca.2020.06.012 [Crossref] [ Google Scholar]
- Henry BM, Aggarwal G, Wong J, Benoit S, Vikse J, Plebani M. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: a pooled analysis. Am J Emerg Med 2020; 38(9):1722-6. doi: 10.1016/j.ajem.2020.05.073 [Crossref] [ Google Scholar]
- Wu MY, Yao L, Wang Y, Zhu XY, Wang XF, Tang PJ. Clinical evaluation of potential usefulness of serum lactate dehydrogenase (LDH) in 2019 novel coronavirus (COVID-19) pneumonia. Respir Res 2020; 21(1):171. doi: 10.1186/s12931-020-01427-8 [Crossref] [ Google Scholar]
- Chan KH, Farouji I, Abu Hanoud A, Slim J. Weakness and elevated creatinine kinase as the initial presentation of coronavirus disease 2019 (COVID-19). Am J Emerg Med 2020;38(7):1548.e1-3. doi: 10.1016/j.ajem.2020.05.015.
- Orsucci D. Is creatine kinase associated with outcome in COVID-19?. Neurosciences 2021; 8(3):216-21. doi: 10.20517/2347-8659.2020.53 [Crossref] [ Google Scholar]
- Akbar MR, Pranata R, Wibowo A, Lim MA, Sihite TA, Martha JW. The prognostic value of elevated creatine kinase to predict poor outcome in patients with COVID-19 - a systematic review and meta-analysis. Diabetes Metab Syndr 2021; 15(2):529-34. doi: 10.1016/j.dsx.2021.02.012 [Crossref] [ Google Scholar]
- Rivas-García S, Bernal J, Bachiller-Corral J. Rhabdomyolysis as the main manifestation of coronavirus disease 2019. Rheumatology (Oxford) 2020; 59(8):2174-6. doi: 10.1093/rheumatology/keaa351 [Crossref] [ Google Scholar]
- Templeton AJ, McNamara MG, Šeruga B, Vera-Badillo FE, Aneja P, Ocaña A. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst 2014; 106(6):dju124. doi: 10.1093/jnci/dju124 [Crossref] [ Google Scholar]
- de Jager CP, van Wijk PT, Mathoera RB, de Jongh-Leuvenink J, van der Poll T, Wever PC. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care 2010; 14(5):R192. doi: 10.1186/cc9309 [Crossref] [ Google Scholar]
- Tamhane UU, Aneja S, Montgomery D, Rogers EK, Eagle KA, Gurm HS. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am J Cardiol 2008; 102(6):653-7. doi: 10.1016/j.amjcard.2008.05.006 [Crossref] [ Google Scholar]
- Park JS, Seo KW, Choi BJ, Choi SY, Yoon MH, Hwang GS. Importance of prognostic value of neutrophil to lymphocyte ratio in patients with ST-elevation myocardial infarction. Medicine (Baltimore) 2018; 97(48):e13471. doi: 10.1097/md.0000000000013471 [Crossref] [ Google Scholar]
- Liu Y, Du X, Chen J, Jin Y, Peng L, Wang HHX. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J Infect 2020; 81(1):e6-12. doi: 10.1016/j.jinf.2020.04.002 [Crossref] [ Google Scholar]
- Hu B, Huang S, Yin L. The cytokine storm and COVID-19. J Med Virol 2021; 93(1):250-6. doi: 10.1002/jmv.26232 [Crossref] [ Google Scholar]
- Tavakolpour S, Rakhshandehroo T, Wei EX, Rashidian M. Lymphopenia during the COVID-19 infection: what it shows and what can be learned. Immunol Lett 2020; 225:31-2. doi: 10.1016/j.imlet.2020.06.013 [Crossref] [ Google Scholar]
- Zhang HJ, Qi GQ, Gu X, Zhang XY, Fang YF, Jiang H. Lymphocyte blood levels that remain low can predict the death of patients with COVID-19. Medicine (Baltimore) 2021; 100(28):e26503. doi: 10.1097/md.0000000000026503 [Crossref] [ Google Scholar]
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020; 323(11):1061-9. doi: 10.1001/jama.2020.1585 [Crossref] [ Google Scholar]
- Fei J, Fu L, Li Y, Xiang HX, Xiang Y, Li MD. Reduction of lymphocyte count at early stage elevates severity and death risk of COVID-19 patients: a hospital-based case-cohort study. Arch Med Sci 2023; 19(5):1303-13. doi: 10.5114/aoms.2020.99006 [Crossref] [ Google Scholar]
- Zou ZY, Ren D, Chen RL, Yu BJ, Liu Y, Huang JJ. Persistent lymphopenia after diagnosis of COVID-19 predicts acute respiratory distress syndrome: a retrospective cohort study. Eur J Inflamm 2021; 19:20587392211036825. doi: 10.1177/20587392211036825 [Crossref] [ Google Scholar]
- Ashtari S, Vahedian-Azimi A, Shojaee S, Pourhoseingholi MA, Jafari R, Bashar FR. Computed tomographic features of coronavirus disease-2019 (COVID-19) pneumonia in three groups of Iranian patients: a single center study. Radiologia (Engl Ed) 2021; 63(4):314-23. doi: 10.1016/j.rxeng.2021.03.003 [Crossref] [ Google Scholar]