J Res Clin Med. 13:34674.
doi: 10.34172/jrcm.025.34674
Review Article
The effect of chlorthalidone on cardiovascular and renal disease: A systematic review
Suryono Suryono Conceptualization, Methodology, Supervision, Writing – review & editing, 1, 2, * 
Hana Nadya Conceptualization, Methodology, Supervision, Writing – review & editing, 3
Wahyu Ikhsan Data curation, Formal analysis, Investigation, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, 1
Achmad Ilham Tohari Data curation, Formal analysis, Investigation, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, 1
Hazbina Fauqi Ramadhan Data curation, Formal analysis, Investigation, Project administration, Resources, Validation, Visualization, Writing – original draft, 4
Author information:
1Department of Cardiology and Vascular Medicine, Faculty of Medicine, University of Jember, East Java, Indonesia
2Department of Cardiology and Vascular Medicine, dr. Soebandi General Hospital, East Java, Indonesia
3Department of Internal Medicine, dr. Soebandi General Hospital, East Java, Indonesia
4Bina Sehat Hospital, East Java, Indonesia
Abstract
Introduction:
Hypertension is a significant risk factor for cardiovascular disease (CVD), including coronary artery disease, cerebrovascular disease, peripheral artery disease, and arteriosclerosis. Hypertension also increases serum creatinine, which is a marker of renal dysfunction. Chlorthalidone (CTDN) is an effective agent for lowering blood pressure in patients with essential hypertension. However, studies have reported adverse events in specific patients, particularly those with cardiovascular and renal diseases. This study aims to evaluate the effects of CTDN on cardiovascular and renal diseases.
Methods:
This study was conducted according to the PRISMA-P guidelines 2015. We systematically searched the PubMed database for keywords related to CTDN, clinical trials, renal dialysis, and hemodialysis. Two independent reviewers selected the studies and extracted the data.
Results:
There were 22 articles included in this study: 17 articles about CTDN and CVDs, and 5 articles about CTDN and renal diseases. This study showed variable results among the published articles. CTDN seems to have a good effect in preventing CVDs, cardiac remodeling, and decreasing blood pressure. However, physicians should consider the potential adverse events that may occur, including hypokalemia, hyponatremia, hyperuricemia, and an increase in serum creatinine levels.
Conclusion:
CTDN has a beneficial effect on CVDs. Nonetheless, the use of CTDN in renal diseases should be monitored due to potential adverse events. CTDN may considered inappropriate in cases of severely decreased renal function. Therefore, we recommend that CTDN can be used in patients with hypertension without renal comorbidities.
Keywords: Cardiovascular, Chlorthalidone, Hypertension, Renal
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
There is no specific funding from any institution, company, or government for this research.
Introduction
The WHO global report regarding the increase in hypertension in adults in the European region/Americas and the South-East Asia/Western Pacific region for 30 years from 1990 to 2020 was 302 million to 427 million and 262 million to 640 million, respectively. Furthermore, there has been a 41% increase in the number of hypertensive patients in the European region/Americas. The most significant increase occurred in the Southeast Asia/Western Pacific region of 144%. This emphasizes the need to control hypertension, especially in the South-East Asia/Western Pacific region1.
Hypertension is a common risk factor for cardiovascular disease (CVD).2 In 2019, the CVD death rate caused by hypertension in adults increased by 43%, with the leading causes of death being ischemic heart disease and respectively.3 Apart from being a risk factor for CVD, hypertension is also a risk factor for renal disease that causes an increase in serum creatinine as a marker of renal dysfunction. Many large-scale observational studies in hypertensive patients have shown that blood pressure is an independent risk factor for renal disease.4 The higher the blood pressure, the greater the risk of chronic kidney disease (CKD) and end-stage renal disease (ESRD). The relationship between blood pressure and CKD is more complex because renal disease itself can increase blood pressure, so it is often difficult to conclude whether CKD is caused solely by hypertension or due to primary renal disease, which causes hypertension, or a combination of both. CKD affects 9% of the world’s population, with a prevalence ranging from 8% to 16% in low-income countries as of 2017. The death rate caused by CKD over the last three decades has increased rapidly by around 41%.5
One way to control hypertension is by administering antihypertensive drugs. Thiazide and thiazide-like diuretics like chlorthalidone (CTDN) have become one of the recommended first pharmacological therapies as antihypertensive drugs.4,6 In recent years, new observations and approaches have emerged to treat hypertension in patients with CKD and to reduce the incidence of CVD. The publication was conducted on a randomized controlled study between placebo and CTDN. CTDN can effectively reduce blood pressure in stage 4 CKD patients.5 There is still very little literature regarding the use of CTDN as antihypertensive therapy and the guidelines from WHO as the first choice of antihypertensive therapy still use the ACEI/ARB group. In contrast, many benefits can be obtained if CTDN is the first choice drug as an antihypertensive and can prevent CVD. However, several studies reported the adverse events of CTDN in specific patients, especially in the case of patients with renal diseases. Therefore, this study aims to systematically evaluate the effects of CTDN on cardiovascular and renal diseases.
Methods
This systematic review was developed following the PRISMA-P 2015 guidelines (Preferred Reporting Items for Systematic Review and Meta-analysis Protocols).7 The primary research query for this systematic review was to assess the impact of CTDN on cardiovascular and renal diseases. We aimed to investigate studies involving any use of CTDN in adult patients, including reported cardiovascular and renal outcomes, especially chronic renal disease, diuretic side effects, and complications of therapy. The keywords consist of ‘’Cardiovascular’’ or ‘’Chronic Renal Disease’’ with ‘and’ Boolean logic to combine with ‘’Chlorthalidone”. There were no restrictions on the country of origin and year of publication. The inclusion criteria were research papers published in English and full-text availability based on the database literature search. The exclusion criteria were review articles, guidelines, commentary, and letter publication types. The literature search was performed on June 30, 2023. Detailed keywords are shown in Supplementary file 1. Additional literature was explored using hand searching that identified the relevant literature in the citation of included studies.
Study selection and quality assessment
The study entries from those queries have been combined into Rayyan.ai, and duplicates have been removed.8 The entries were then methodically screened to remove those without an abstract, those with a publication type of letter or correspondence, and those irrelevant to the primary search query. Two independent reviewers (WI and AIT) evaluated the full-text articles to exclude review articles, case reports, qualitative surveys, fundamental science, and diagnostic testing publications. Two reviewers also independently assessed the methodological quality of included studies using the Newcastle-Ottawa Scale (NOS) for quality assessment of non-randomized studies in systematic reviews and meta-analyses.7 The NOS is composed of three primary domains: comparability (comparing study groups), outcome (evaluating the study’s findings), and selectivity (choosing the study population). Each study receives an overall score of up to nine points on the NOS scale, which indicates the methodological quality of the study. Data extraction was created with the following headings: author, year of publication, study patient population size, study type, duration of follow-up, and study conclusion.
Results
Systematic review findings
The initial screen generates 26 articles on PubMed and 14 articles from hand searching (Figure 1). After exclusion from irrelevant studies and applying inclusion criteria, 22 references were obtained where CTDN, a diuretic and anti-hypertensive drug, was associated with cardiovascular events and its effect on the renal (Figure 1). The summary of the NOS quality assessment is presented in Table 1. There are 3 references discussing the benefits of CTDN, 3 references discussing the side effects of using CTDN on CVD, 11 references discussing comparisons of CTDN with other antihypertensive drugs, and 5 references discussing the effects of CTDN on the kidney (Table 2).
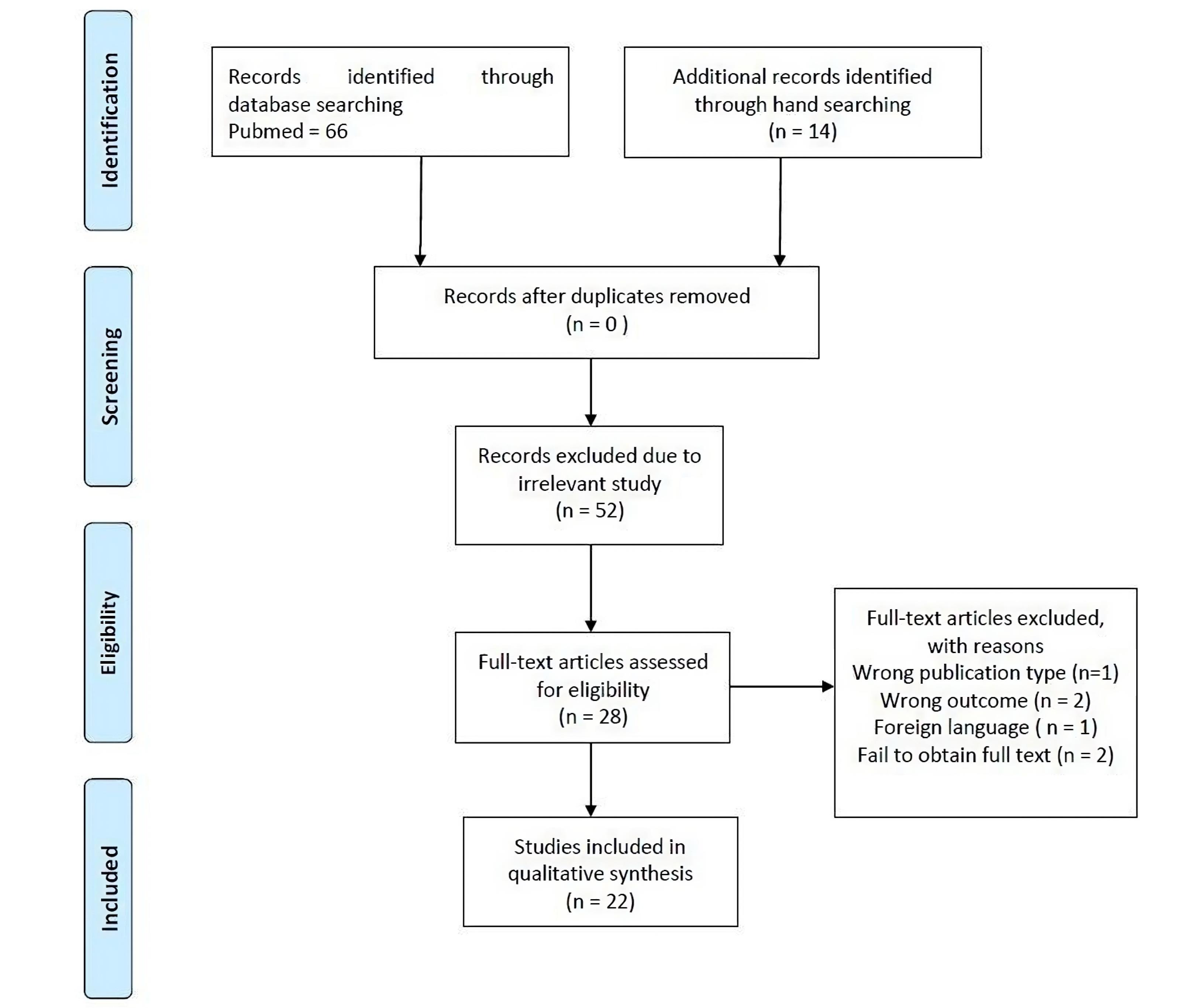
Figure 1.
PRISMA flow chart of chlorthalidone and cardiovascular–renal diseases
.
PRISMA flow chart of chlorthalidone and cardiovascular–renal diseases
Table 1.
Newcastle Ottawa Scale (NOS) of included studies
|
First author, year
|
Selection
|
Comparability
|
Outcome
|
NOS
|
|
Effects of chlorthalidone on cardiovascular diseases
|
| Geza Simon, 19919 |
*** |
* |
*** |
7 |
| Philip R. Liebson, 199510 |
*** |
* |
*** |
7 |
| Drago Rakić, 200211 |
** |
* |
*** |
6 |
| ALLHAT, 200212 |
** |
* |
*** |
6 |
| ALLHAT, 200313 |
** |
* |
*** |
6 |
| Ettore Malocco, 200314 |
*** |
* |
*** |
7 |
| Michael E. Erns, 200615 |
** |
* |
*** |
6 |
| Anil K. Pareek, 200916 |
** |
* |
*** |
6 |
| Michael P. Dorsch, 201117 |
*** |
* |
*** |
7 |
| John B Kostis, 201118 |
**** |
* |
*** |
8 |
| Georg L. Bakris, 201219 |
** |
* |
*** |
6 |
| Irfan A. Dhalla, 201320 |
*** |
* |
*** |
7 |
| Beom June Kwon, 201321 |
*** |
* |
*** |
7 |
| Joseph J. Saseen, 201422 |
** |
* |
*** |
6 |
| Anil K. Pareek, 201623 |
** |
* |
*** |
6 |
| Carolina Bertoluci, 201724 |
** |
* |
*** |
6 |
| George Hripcsak, 202025 |
** |
* |
*** |
6 |
|
Effects of chlorthalidone on renal diseases
|
| Elliot, 200626 |
** |
* |
*** |
6 |
| Rajiv Agarwal, 201427 |
** |
* |
*** |
6 |
| Joshua I. Bazirlay, 201828 |
*** |
* |
*** |
7 |
| Rajiv Agarwal, 202129 |
**** |
* |
*** |
8 |
| Cedric Edwards, 202130 |
*** |
* |
*** |
7 |
Table 2.
The characteristics of the included studies
|
First author
|
Year of publication
|
Design
|
Sample size
|
Treatment
|
Follow-up
|
Results
|
|
Effects of chlorthalidone on cardiovascular diseases
|
| Geza Simon9 |
1991 |
Double-blind, placebo-controlled, randomized clinical trial |
4736 |
CTDN 12.5 mg, 25 mg;
Placebo |
4.5 years |
CTDN low dose 12.5 mg reduces the incidence of stroke by 36% |
| Philip R. Liebson10 |
1995 |
Randomized, double-blind clinical trial |
902 |
CTDN 12.5 mg; Acebutolol 400 mg; Doxazosin 1 mg, 2 mg; Amlodipine 5 mg; Enalapril 5 mg; |
4 years |
CTDN has a greater effect on reducing left ventricular mass compared to acebutolol, doxazosin, amlodipine, enalapril |
| Drago Rakie11 |
2002 |
A randomized, double-blind, prospective study |
64 |
Indapamide 2.5 mg; Nicardipine 20 mg; Propranolol 40 mg; CTDN 25 mg |
6 months |
CTDN reduced left ventricular mass, whereas left ventricular wall thickness decreased only slightly. Compared with indapamide, nicardipine, and propranolol |
| ALLHAT12 |
2002 |
A randomized, double-blind, active-controlled trial |
33.357 |
CTDN 12.5 mg, 25 mg;
Amlodipin 2.5 mg, 5 mg, 10 mg; Lisinopril 10 mg, 20 mg, 30 mg, 40 mg |
4 to 8 years |
CTDN should be chosen as the first antihypertensive therapy because it is superior in preventing one or more CVD diseases and CTDN has a cheaper price. |
| ALLHAT13 |
2003 |
A randomized, double-blind, active-controlled trial |
9.232 |
CTDN 12.5 mg, 25 mg;
Doxazosin 2 mg, 4 mg, 8 mg |
4 years |
CTDN is superior in preventing more CVD (CHD, stroke, angina, HF, and PAD) and is cheaper than doxazosin |
| Ettore Malacco14 |
2003 |
Retrospective observational cohort study |
1882 |
CTDN 12.5 mg;
Lacidipine 4 mg |
32 months |
CTDN or lacidipine markedly reduced systolic blood pressure with no difference in cardiovascular events and mortality. |
| Michael E. Ernst15 |
2006 |
A randomized, single-blinded |
54 |
CTDN 12.5 mg, 25 mg;
HCTZ 25 mg, 50 mg |
8 weeks |
CTDN is more effective in reducing systolic blood pressure compared to HCTZ |
| Anil Pareek16 |
2009 |
Randomized, comparative, multicenter, open-label study |
137 |
CTDN 6.25 mg, 12.5 mg;
HCTZ 12.5 mg;
Losartan 25 mg, 50 mg |
18 weeks |
The combination of losartan and low-dose CTDN is more effective in lowering blood pressure than the combination of losartan and HCTZ |
| Michael P. Dorsch17 |
2011 |
Retrospective Cohort Study |
6.441 |
CTDN ≤ 50 mg/ > 50 mg
HCTZ ≤ 50 mg/ > 50 mg |
1.5 years |
CTDN is more effective in reducing CVDs than HCTZ |
| John B Kortis18 |
2011 |
A randomized, placebo-controlled and clinical trial |
4.736 |
CTDN 12.5 mg, 25 mg;
Placebo |
22 years |
CTDN at 4.5 years had significantly lower mortality after 22 years of follow-up. |
| Georg L. Bakris19 |
2012 |
Randomized, double-blind, double-dummy |
609 |
CTDN 12,5 mg; 25 mg
Azilsartan 40 mg |
10 weeks |
CTDN combined with azilsartan medoxomil lowered blood pressure more effectively than the combination of HCTZ with azilsartan medoxomil. |
| Irfan A. Dhalla20 |
2013 |
Observational cohort study |
29.837 |
CTDN 12,5 mg; 25 mg; 50 mg
HCTZ 12,5 mg; 25 mg; 50 mg |
5 years |
CTDN in elderly patients has no association with events or death compared to HCTZ. However, it is associated with the incidence of electrolyte abnormalities, especially hypokalemia |
| Beom-June Kwon21 |
2013 |
Open-label, randomized, prospective cross-over study |
28 |
CTDN 12.5 mg;
HCTZ 25 mg;
Candesartan 8 mg |
8 weeks |
The combination of CTDN with Candesartan has a significant decrease in PWV compared to the combination of HCTZ with Candesartan |
| Joseph J. Saseen22 |
2015 |
Retrospective cohort analysis study |
428 |
CTDN 25 mg;
HCTZ 25 mg, 50 mg |
7 years |
CTDN has a better response in reducing systolic and diastolic blood pressure than HCTZ, but CTDN has a hypokalemic effect compared to HCTZ |
| Anil K. Pareek23 |
2016 |
Double-blind, double dummy, randomized, parallel group, comparative, multicentric study |
54 |
CTDN 6.25 mg;
HCTZ 12.5 mg |
12 weeks |
Low-dose CTDN, 6.25 mg, can be used as monotherapy for the treatment of essential hypertension, whereas low-dose HCTZ monotherapy is not an appropriate antihypertensive agent. |
| Carolina Bertoluci24 |
2018 |
Cohort study |
110 |
CTDN 12.5 mg |
1,5 years |
CTDN treatment can assist LA and LV remodeling |
| George Hripcsak25 |
2020 |
Observational, retrospective, and comparative cohort study |
730.225 |
CTDN 12.5 mg;
HCTZ 25 mg |
17 years |
There is no significant difference in effectiveness between CTDN and HCTZ. However, there are differences in safety outcomes, with CTDN being associated with a higher risk of hypokalemia compared with HCTZ. |
|
Effects of chlorthalidone on renal diseases
|
| Elliot26 |
2006 |
A randomized, double-blind, active-controlled trial |
448 |
CTDN 12.5 mg, 25 mg;
Amlodipine 2.5 mg, 5 mg, 10 mg;
Lisinopril 10 mg, 20 mg, 40 mg. |
4 years |
Administration of amlodipine, lisinopril has a higher GFR compared to administration of CTDN |
| Rajiv Agarwal27 |
2014 |
Single arm without a control group |
14 |
Lisinopril 20 mg, 40 mg;
Amlodipine 10 mg;
Torsemide 10 mg, 20 mg;
CTDN 25 mg, 50 mg |
12 weeks |
Biological activity of CTDN in advanced renal diseases have side effects such as hypokalemia, hyponatremia, hyperuricemia, expected transient changes in serum creatinine concentration, and orthostatic hypotension are common |
| Joshua I. Barzilay28 |
2018 |
Randomized double-blind active-controlled |
20.707 |
CTDN N/A; Amlodipine N/A; Lisinopril N/A |
2 years |
CTDN was associated with a higher estimated decrease in glomerular filtration rate compared with use of amlodipine or lisinopril. CTDN is more protective against heart failure than lisinopril or amlodipine |
| Rajiv Agarwal29 |
2021 |
Double-blind, randomized, placebo-controlled trial |
160 |
CTDN 12.5 mg, 25 mg, 50 mg;
Placebo |
12 weeks |
CTDN administration results in a reversible increase in serum creatinine, hypokalemia, hyperglycemia and hyperuricemia. |
| Cedric Edwards30 |
2021 |
Retrospective cohort study |
12.722 |
CTDN ≤ 12.5 mg, > 12.5 mg ≤ 25 mg, > 25 mg;
HCTZ ≤ 37.5 mg, > 37.5 mg ≤ 75 mg, > 75 mg |
8 weeks |
Use of CTDN was associated with a reduced risk of eGFR ( ≥ 30%) which is higher and hypokalemia compared to the use of hydrochlorothiazide. |
CHD: Congestive heart failure; CTDN: Chlorthalidone; CVD: Cardiovascular diseases; HCTZ: Hydrochlorothiazide; LA: Left atrium; LV: Left ventricle; N/A: Not available; GFR: Glomerulus filtration rate; eGFR: Estimation glomerulus filtration rate.
The effect of chlorthalidone on cardiovascular conditions
As illustrated in Table 2, the included studies show promising effects on the use of CTDN for CVD. Many studies compare the effectiveness of CTDN and other antihypertensive drugs such as HCTZ, calcium channel blockers, and beta-blockers. Half of the studies (8 out of 16, 50%) reported that CTDN was more effective in reducing systolic blood pressure and diastolic blood pressure than other antihypertensive drugs. So, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure recommends CTDN as the first-line treatment of uncomplicated hypertension and no comorbidities.23 Moreover, 3 of 16 studies (18.75%) reported a greater effect of CTDN in reducing LV mass and remodeling in the LA and LV compared to other antihypertensive drugs. On the other hand, 3 of 16 studies (18.75%) reported the effect of CTDN as a therapy to prevent and reduce CVD (CHD, stroke, angina, HF, and PAD). On the other hand, 2 of 16 studies (12.5%) reported that CTDN had lower side effects on the incidence of hypokalemia compared to HCTZ. The results showed promising effects on the use of CTDN for CVDs.
The effect of chlorthalidone on renal disease
Based on table 2 which states the effect of CTDN on kidney disease. The majority of studies (3 out of 5, 60%) have evaluated CTDN’s impact on the incidence of electrolyte imbalance: hypokalemia, hyponatremia; hyperglycemia; and hyperuricemia. On the other hand, 2 out of 5 studies (40%) reported that the use of CTDN can increase eGFR. Therefore, the use of CTDN must pay attention to kidney disease in patients.
Discussion
This study provides updated evidence regarding the usage of CTDN in hypertension therapy. CTDN is a diuretic derived from the sulfonamide group such as thiazides because it has the same functional group as hydrochlorothiazide (HCTZ), so it is often called diuretic-like thiazide.31 Although often referred to as diuretic-like thiazide, the pharmacokinetic and pharmacodynamic modes of action of CTDN and HCTZ are very different. The first reason CTDN is distinguished from HCTZ is because CTDN has a long half-life of around 40 hours, while HCTZ is only 6-9 hours. The cause of the long CTDN half-life is after CTDN enters the body and is immediately concentrated in the erythrocytes. A study states that CTDN is concentrated 7-10 times more in erythrocytes than plasma.32 The mechanism of action of CTDN involves inhibiting Na + /Cl - co-transporter (NCC) in the luminal membrane of the distal convoluted tubule of the renal. The NCC is responsible for about 5-7% of total sodium reabsorption or 130 mmol/day in the nephron.20
The results showed that CTDN has beneficial effects on the cardiovascular system, such as decreasing systolic and diastolic blood pressure, cardiac remodeling, and preventing CVD. The effect of CTDN on reducing blood pressure is explained by Davis in 2012 explained HCTZ and CTDN are more effective in lowering blood pressure than other diuretics but have less ability to affect patients with volume overload. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure recommends CTDN as the first-line treatment of uncomplicated hypertension and no comorbidities.16 Reduced sodium reabsorption increases the amount of urine output, thereby reducing circulating blood volume and lowering blood pressure.
This systematic review demonstrated the effect of CTDN on cardiovascular events by lowering blood pressure in hypertensive patients. The result of this decrease in blood pressure impacts reducing the LV mass. Strengthening the explanation of the effect of CTDN on reducing LVM, Liebson et al compared five types of antihypertensives including diuretic (CTDN), β-blocker (acebutolol), α-antagonist (doxazosin mesylate), calcium antagonist (amlodipine maleate), and angiotensin-converting enzyme inhibitor (enalapril maleate). All antihypertensives demonstrated a 10% to 15% reduction in LVM. However, the CTDN group experienced the greatest effect on reducing LVM with an average of around 35 grams after giving CTDN for 12 months.10 Besides impacting the mass in the LV, CTDN was found to be more effective than HCTZ in reducing the risk of patients with cardiovascular events.
A secondary analysis of a randomized clinical trial of mortality and morbidity in individuals receiving antihypertensive medications diuretic-like-thiazide (CTDN), ACE inhibitors, and calcium channel blockers explained that CTDN as an antihypertensive is more effective in reducing CVD than ACE Inhibitors. Compared with CTDN, the ACE Inhibitors group had a 19% higher risk of death from stroke.33
Besides CVD, CTDN is also helpful in reducing morbidity rates from cerebrovascular disease. The SHEP cooperative research group also explained the effect of CTDN on the incidence of stroke. There were several adverse events following treatment with CTDN. The use of CTDN was associated with an increase in electrolyte and renal disorders, including hypokalemia, hyponatremia, acute renal failure, and chronic renal disease. Based on electrolyte findings, CTDN’s association with an increase in the incidence of type II diabetes may be related to potassium depletion or dehydration.34 Current literature shows that CTDN has different results in lowering blood pressure in patients with renal diseases. Many studies support that CTDN effectively reduces blood pressure in patients with CKD.15,19,25 Thiazide-like diuretics have also been reported to have renoprotective properties. CTDN administration could decrease urine albumin excretion, according to results from the CLICK study and its pilot phase, designed to treat patients with severe CKD.30
Besides electrolyte imbalance, CTDN also affects the estimated glomerulus filtration rate (eGFR). This was explained by Barzilay et al that CTDN had a much higher rate of decrease in eGFR compared to the use of amlodipine and lisinopril.27 CTDN may be used in case of hypertension, but the adverse event should be monitored in each comorbidity. This systematic review has limitations that cannot determine which dose has a blood pressure-lowering effect with fewer adverse events. Therefore, future research can be conducted to explore the effect in different populations, comorbidities, dose ranges, and longer follow-ups to monitor the long-term effects of using CTDN in individuals with hypertension without renal disease. This study has some limitations. Our study only analyzed literature published in English; the findings of this study may not combine other studies published in other languages. The systematic review in this study was only conducted in the PubMed database; further studies that evaluate the evidence in other databases are needed in the future.
Study Highlights
What is current knowledge?
-
Based on the theory to date, there is a correlation between cardiac and renal disease, called cardiorenal syndrome, which may affect each other. Therefore, it is important to discuss the treatment of heart or renal diseases based on both perspectives.
-
Chlorthalidone is not included in the newest guideline for hypertension and is not commonly used lately.
What is new here?
-
Even though chlorthalidone is not included in the latest guidelines, many studies suggest that chlorthalidone has an antiremodeling effect for cardiac disease, the same as ace and arb. However, the effects of chlorthalidone on the kidneys are still controversial.
Conclusion
CTDN has a beneficial effect on lowering blood pressure, preventing CVDs, and cardiac remodeling. However, the use of CTDN in renal disease should be monitored because of its side effects. CTDN should not be given if there is a severe decline in renal function. Therefore, we recommend that CTDN can be used in case of hypertension without renal comorbidities.
Competing Interests
The authors declare there is no conflict of interest related to the publication of this work.
Data Availability Statement
All data in this study were available in the manuscript. Further information may be asked to the corresponding author.
Ethical Approval
Ethical approval and informed consent were not required for this study, as these studies were based on previously published articles.
Ethical Approval
This study does not need ethical approval because the authors did not include any human or animal subjects in this review
Supplementary Files
Supplementary file 1. Keywords in PubMed database.
(pdf)
Acknowledgements
We would like to thank the department of Cardiology and Vascular Medicine, dr. Soebandi General Hospital and Faculty of Medicine, Jember University for giving invaluable support for the authors.
References
- Kario K, Okura A, Hoshide S, Mogi M. The WHO Global report 2023 on hypertension warning the emerging hypertension burden in globe and its treatment strategy. Hypertens Res 2024; 47(5):1099-102. doi: 10.1038/s41440-024-01622-w [Crossref] [ Google Scholar]
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation 2018; 137(12):e67-492. doi: 10.1161/cir.0000000000000558 [Crossref] [ Google Scholar]
- Liu J, Bu X, Wei L, Wang X, Lai L, Dong C. Global burden of cardiovascular diseases attributable to hypertension in young adults from 1990 to 2019. J Hypertens 2021; 39(12):2488-96. doi: 10.1097/hjh.0000000000002958 [Crossref] [ Google Scholar]
- Sazlina SG, Sooryanarayana R, Ho BK, Omar MA, Krishnapillai AD, Mohd Tohit N. Cardiovascular disease risk factors among older people: data from the National Health and Morbidity Survey 2015. PLoS One 2020; 15(10):e0240826. doi: 10.1371/journal.pone.0240826 [Crossref] [ Google Scholar]
- Burnier M, Damianaki A. Hypertension as cardiovascular risk factor in chronic kidney disease. Circ Res 2023; 132(8):1050-63. doi: 10.1161/circresaha.122.321762 [Crossref] [ Google Scholar]
- Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D. 2020 International Society of Hypertension global hypertension practice guidelines. Hypertension 2020; 75(6):1334-57. doi: 10.1161/hypertensionaha.120.15026 [Crossref] [ Google Scholar]
- Kamioka H. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Jpn Pharmacol Ther 2019; 47(8):1177-85. [ Google Scholar]
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev 2016; 5(1):210. doi: 10.1186/s13643-016-0384-4 [Crossref] [ Google Scholar]
- Simon G. Prevention of stroke in older persons with isolated systolic hypertension. JAMA 1991; 266(20):2829-30. doi: 10.1001/jama.1991.03470200041012 [Crossref] [ Google Scholar]
- Liebson PR, Grandits GA, Dianzumba S, Prineas RJ, Grimm RH Jr, Neaton JD. Comparison of five antihypertensive monotherapies and placebo for change in left ventricular mass in patients receiving nutritional-hygienic therapy in the Treatment of Mild Hypertension Study (TOMHS). Circulation 1995; 91(3):698-706. doi: 10.1161/01.cir.91.3.698 [Crossref] [ Google Scholar]
- Rakić D, Rumboldt Z, Bagatin J, Polić S. Effects of four antihypertensive monotherapies on cardiac mass and function in hypertensive patients with left ventricular hypertrophy: randomized prospective study. Croat Med J 2002; 43(6):672-9. [ Google Scholar]
- ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting
enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent
Heart Attack Trial (ALLHAT). JAMA. 2002;288(23):2981-97. doi: 10.1001/jama.288.23.2981.
- Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial Collaborative Research Group. Diuretic versus alpha-blocker as first-step antihypertensive therapy: final results from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Hypertension. 2003;42(3):239-46. doi: 10.1161/01.Hyp.0000086521.95630.5a.
- Malacco E, Mancia G, Rappelli A, Menotti A, Zuccaro MS, Coppini A. Treatment of isolated systolic hypertension: the SHELL study results. Blood Press 2003; 12(3):160-7. doi: 10.1080/08037050310009545 [Crossref] [ Google Scholar]
- Ernst ME, Carter BL, Goerdt CJ, Steffensmeier JJ, Phillips BB, Zimmerman MB. Comparative antihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension 2006; 47(3):352-8. doi: 10.1161/01.HYP.0000203309.07140.d3 [Crossref] [ Google Scholar]
- Pareek A, Basavanagowdappa H, Zawar S, Kumar A, Chandurkar N. A randomized, comparative study evaluating the efficacy and tolerability of losartan-low dose chlorthalidone (625 mg) combination with losartan-hydrochlorothiazide (125 mg) combination in Indian patients with mild-to-moderate essential hypertension. Expert Opin Pharmacother 2009; 10(10):1529-36. doi: 10.1517/14656560902991514 [Crossref] [ Google Scholar]
- 17Dorsch MP, Gillespie BW, Erickson SR, Bleske BE, Weder AB. Chlorthalidone reduces cardiovascular events compared with hydrochlorothiazide: a retrospective cohort analysis. Hypertension 2011; 57(4):689-94. doi: 10.1161/hypertensionaha.110.161505 [Crossref] [ Google Scholar]
- Kostis JB, Cabrera J, Cheng JQ, Cosgrove NM, Deng Y, Pressel SL. Association between chlorthalidone treatment of systolic hypertension and long-term survival. JAMA 2011; 306(23):2588-93. doi: 10.1001/jama.2011.1821 [Crossref] [ Google Scholar]
- Bakris GL, Sica D, White WB, Cushman WC, Weber MA, Handley A, et al. Antihypertensive efficacy of hydrochlorothiazide vs chlorthalidone combined with azilsartan medoxomil. Am J Med 2012;125(12):1229.e1-1229.e10. doi: 10.1016/j.amjmed.2012.05.023.
- Dhalla IA, Gomes T, Yao Z, Nagge J, Persaud N, Hellings C. Chlorthalidone versus hydrochlorothiazide for the treatment of hypertension in older adults: a population-based cohort study. Ann Intern Med 2013; 158(6):447-55. doi: 10.7326/0003-4819-158-6-201303190-00004 [Crossref] [ Google Scholar]
- Kwon BJ, Jang SW, Choi KY, Kim DB, Cho EJ, Ihm SH. Comparison of the efficacy between hydrochlorothiazide and chlorthalidone on central aortic pressure when added on to candesartan in treatment-naïve patients of hypertension. Hypertens Res 2013; 36(1):79-84. doi: 10.1038/hr.2012.143 [Crossref] [ Google Scholar]
- Saseen JJ, Ghushchyan V, Nair KV. Comparing clinical effectiveness and drug toxicity with hydrochlorothiazide and chlorthalidone using two potency ratios in a managed care population. J Clin Hypertens (Greenwich) 2015; 17(2):134-40. doi: 10.1111/jch.12453 [Crossref] [ Google Scholar]
- Pareek AK, Messerli FH, Chandurkar NB, Dharmadhikari SK, Godbole AV, Kshirsagar PP. Efficacy of low-dose chlorthalidone and hydrochlorothiazide as assessed by 24-h ambulatory blood pressure monitoring. J Am Coll Cardiol 2016; 67(4):379-89. doi: 10.1016/j.jacc.2015.10.083 [Crossref] [ Google Scholar]
- Bertoluci C, Foppa M, Santos ABS, Branchi TV, Fuchs SC, Fuchs FD. Echocardiographic left ventricular reverse remodeling after 18 months of antihypertensive treatment in stage I hypertension Results from the Prever-Treatment Study. Am J Hypertens 2018; 31(3):321-8. doi: 10.1093/ajh/hpx171 [Crossref] [ Google Scholar]
- Hripcsak G, Suchard MA, Shea S, Chen R, You SC, Pratt N. Comparison of cardiovascular and safety outcomes of chlorthalidone vs hydrochlorothiazide to treat hypertension. JAMA Intern Med 2020; 180(4):542-51. doi: 10.1001/jamainternmed.2019.7454 [Crossref] [ Google Scholar]
- Elliott WJ. Renal outcomes in high-risk hypertensive patients treated with an angiotensin-converting enzyme inhibitor or a calcium channel blocker vs a diuretic: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Yearbook of Cardiology. 2006(Suppl 1):64-6. doi: 10.1016/s0145-4145(07)70036-9.
- Agarwal R, Sinha AD, Pappas MK, Ammous F. Chlorthalidone for poorly controlled hypertension in chronic kidney disease: an interventional pilot study. Am J Nephrol 2014; 39(2):171-82. doi: 10.1159/000358603 [Crossref] [ Google Scholar]
- Barzilay JI, Davis BR, Pressel SL, Ghosh A, Rahman M, Einhorn PT. The effects of eGFR change on CVD, renal, and mortality outcomes in a hypertensive cohort treated with 3 different antihypertensive medications. Am J Hypertens 2018; 31(5):609-14. doi: 10.1093/ajh/hpx223 [Crossref] [ Google Scholar]
- Agarwal R, Sinha AD, Cramer AE, Balmes-Fenwick M, Dickinson JH, Ouyang F. Chlorthalidone for hypertension in advanced chronic kidney disease. N Engl J Med 2021; 385(27):2507-19. doi: 10.1056/NEJMoa2110730 [Crossref] [ Google Scholar]
- Edwards C, Hundemer GL, Petrcich W, Canney M, Knoll G, Burns K. Comparison of clinical outcomes and safety associated with chlorthalidone vs hydrochlorothiazide in older adults with varying levels of kidney function. JAMA Netw Open 2021; 4(9):e2123365. doi: 10.1001/jamanetworkopen.2021.23365 [Crossref] [ Google Scholar]
- Jaques DA, Péchère-Bertschi A, Ponte B. Chlortalidone: outdated or reborn?. Cardiovasc Med 2016; 19(12):322-7. [ Google Scholar]
- Sica DA. Chlorthalidone: has it always been the best thiazide-type diuretic?. Hypertension 2006; 47(3):321-2. doi: 10.1161/01.HYP.0000203147.75714.ba [Crossref] [ Google Scholar]
- Yamal JM, Martinez J, Osani MC, Du XL, Simpson LM, Davis BR. Mortality and morbidity among individuals with hypertension receiving a diuretic, ACE inhibitor, or calcium channel blocker: a secondary analysis of a randomized clinical trial. JAMA Netw Open 2023; 6(12):e2344998. doi: 10.1001/jamanetworkopen.2023.44998 [Crossref] [ Google Scholar]
- Agarwal R. Should we CLICK on chlorthalidone for treatment-resistant hypertension in chronic kidney disease?. Clin Kidney J 2023; 16(5):793-6. doi: 10.1093/ckj/sfac272 [Crossref] [ Google Scholar]