J Res Clin Med. 13:34611.
doi: 10.34172/jrcm.025.34611
Original Article
Comparing clinic-supervised and internet-based exercise therapy: A randomized controlled trial on pain, range of motion, and physical function in knee osteoarthritis patients
Azar Moezy Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing, 1, * 
Bita Zoghalchi Data curation, Investigation, Methodology, Validation, Visualization, 1
Ahmad Nazari Formal analysis, Supervision, Validation, Visualization, 1
Arezoo Abasi Formal analysis, Software, Writing – original draft, 2
Author information:
1Department of Sports and Exercise Medicine, School of Medicine, Iran University of Medical Sciences, Tehran, Iran
2Department of Health Information Management, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran
Abstract
Introduction:
Knee osteoarthritis (KOA) stands out as the most common synovial joint disease among people, leading to a reduced quality of life, persistent pain, muscle weakness, and significant functional impairments. The aim of this study is to carry out an investigation that assesses the efficacy of clinic-supervised and internet-based exercise therapy (IET) on pain, range of knee flexion, and physical function of patients with KOA.
Methods:
This randomized controlled trial enrolled 54 patients between the ages of 50 and 75, all of whom had confirmed KOA. These patients were randomly allocated to one of two groups, both of which underwent 18 sessions of exercise therapy. One group received supervised therapy, while the other received therapy delivered via the internet. The study measured various outcomes, including pain intensity assessed with the VAS, thigh girth (TG), knee active flexion range of motion (FROM), the six-minute walk test (6MWT), the timed up and go test (TUG), and knee functionality evaluated using the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) questionnaire, both before and after the intervention. We used the paired t-test for intra-group analysis and the independent samples t-test and analysis of covariance (ANCOVA) test to compare differences between the groups.
Results:
Significant differences in outcomes were observed before and after the intervention in both groups (P=0.001). However, the ANCOVA test revealed no significant differences between the groups following the study. The statistical analysis, performed with an independent-samples t-test, indicated no significant differences between the two groups concerning VAS, active knee flexion, thigh girth, and WOMAC scores, suggesting that both supervised exercise therapy (SET) and IET protocols yielded similar effectiveness. Nevertheless, when employing the independent-samples t-test, there were significant differences between the groups in the TUG (P=0.001) and the 6MWT (P=0.017), with the IET group demonstrating superior performance.
Conclusion:
The results of this study indicate that both SET and IET produce comparable outcomes in terms of reducing pain, increasing thigh girth, increasing knee flexion range, and improving WOMAC scores and the physical function of patients with KOA. The internet-based approach may offer added convenience and motivation for patients.
Keywords: Exercise therapy, Knee, Osteoarthritis, Pain, WOMAC questionnaire
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
No funding has been received to report.
Introduction
Knee Osteoarthritis (KOA) involves the gradual loss of joint cartilage, causing joint stiffness, limited range of motion, knee-buckling, reduced physical function, and decreased quality of life in around one-third of individuals aged 65 and above.1-3 With the global population aging and sedentary lifestyles becoming more prevalent, KOA has become the second leading contributor to global disability.4 In Iran's urban population, KOA's prevalence is increasing, particularly among those aged 40 and above, with a significant rate of 41.9%.5 The impact is more significant among women, influenced by lifestyle choices and risk factors, with a prevalence of 60.5%, compared to 38.6% in men, and the highest occurrence is seen in individuals with a BMI exceeding 30.6,7
Functional disabilities in KOA patients primarily result from the weakness of the knee extensor muscles, especially in those with severe knee pain. This weakness exacerbates cartilage deterioration.8 In the initial stages of KOA, patients experience muscle atrophy, strength deficiencies ranging from 20%-45%, and impaired muscle function. These factors limit the quadriceps femoris (QF) muscle's capacity to generate necessary force, crucial for joint stabilization and shock absorption during walking.9 Consequently, this constraint results in pain, swelling and abnormal distribution of loading within the knee.10 Therefore, strengthening the QF is crucial in conservative KOA treatment, offering substantial therapeutic benefits.11,12 Despite strong recommendations for KOA patients to engage in physical exercises, many maintain inactive lifestyles. Obstacles like limited access to healthcare services, particularly for those with financial constraints, contribute to low adherence to exercise routines. This leads to challenges in reaching appropriate specialists and supervised exercise therapy (SET) programs.2,11,13-15 Emerging approaches, such as SET and internet-based exercise therapy (IET), are recognized for alleviating pain and enhancing functionality in KOA patients.
Conventional SET administered in clinical environments has played a pivotal role in conservative KOA treatment, involving specific exercise regimens overseen by a specialist.16-19 However, advancements in technology and increased internet connectivity have provided a new avenue for exercise therapy delivery. Online rehabilitation offers the convenience of remotely accessing tailored exercise programs, potentially improving healthcare accessibility and addressing geographical and scheduling limitations. Internet-based rehabilitation also presents a cost-effective alternative for providing instructions and monitoring exercise protocols.20,21
Through a systematic review, Cottrell et al emphasized the effectiveness of telerehabilitation in contrast to conventional methods for improving physical function and reducing pain in individuals with musculoskeletal conditions. Because this approach is relatively new, additional research is required to delve deeper into its impact.22
Allen et al demonstrated the efficacy of IET programs in improving symptoms of KOA and increasing patient satisfaction with this approach.20
As Iran's elderly population increases, and chronic musculoskeletal conditions prevail, the demand for specialized rehabilitation services and exercise therapy is rising.23 The COVID-19 pandemic and increased vulnerability of the elderly have led to challenges for conventional clinic-centered treatment methods, emphasizing the need for alternatives like IET to meet musculoskeletal rehabilitation demands. This situation prompted an investigation into the effectiveness of IET. In this research, we delve into the evolving landscape of KOA management, considering the historical context of SET and the innovative potential of IET. By critically evaluating the existing literature and conducting empirical research, we provide a nuanced perspective of the comparative effectiveness of these two approaches. Ultimately, this research emphasizes the importance of customizing interventions to meet patients' needs and preferences, while also pushing forward the discussion about the optimal way to deliver exercise therapy and supervision for KOA patients.
Methods
Design
The study was an assessor-blind randomized controlled trial, with patients randomly assigned to two different exercise therapy intervention groups; SET and IET.
Participants
The study included 54 female patients referred to Hazrat-e Rasool hospital in Iran University of Medical Sciences, from 2021 to 2022.
These patients had confirmed primary KOA, diagnosed using the American College of Rheumatology criteria through clinical history, physical exams, and radiographic assessments. The study's inclusion criteria were: (1) diagnosis of KOA at stages II and III, as determined by the Kellgren and Lawrence classification based on X-ray findings; (2) participants aged between 50 and 75 years; (3) BMI of 30 or lower; (4) a history of knee pain for at least 6 months, rated at least 3 on the visual analog scale (VAS) during activities like stair climbing and squatting; (5) participants in the IET group needed to be well-versed in the use of social networks, particularly WhatsApp messenger; (6) a normal mental condition.
The exclusion criteria included the following:
-
Previous surgeries or injuries involving the knee or lower limbs;
-
Presence of cancerous tumors, neuromuscular disorders and bone implants;
-
History of lower limb fractures occurring in the last 6 months;
-
History of acute traumatic or chronic injuries, or any conditions that may influence the study;
-
Involvement in exercise programs or physical therapy within the last three months;
-
Intra-articular injections received in the past six months;
-
Use of opioid, pain relievers or systemic corticosteroids within the last 4 weeks;
-
Inability to perform exercises due to significant pain or other restrictions;
-
Lack of interest in participating in the study;
-
Incomplete assessments or treatment protocols.
Sample size
Each group comprised 24 participants, determined based on a significance level (α) of 0.05 and a type II error rate (β) of 0.20 (80% power). This sample size was calculated to detect a two-point difference in VAS pain scores.24 To accommodate possible dropouts, the sample size was raised to 27 patients in each group.
Study settings
Eligible patients were initially evaluated by a specialist to determine their suitability for the study. After this, participants completed a baseline assessment that involved using a VAS to measure pain levels, assessing active knee flexion range of motion (FROM), performing six-minute walk test (6MWT) and time up and go (TUG) functional tests, measuring thigh girth (TG), and completing the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire. These measurements were taken both before the intervention and after the 6-week intervention period.
Randomized allocation
Initially, 68 patients were enrolled in the study in accordance with the ethical standards. After excluding seven participants who failed to meet the eligibility criteria, 61 individuals were randomly assigned to either the SET or IET group, through computer-generated randomization (see Figure 1). The assessors who evaluated the participants were blinded to the group assignments, maintaining the integrity of the study’s blinding procedure.
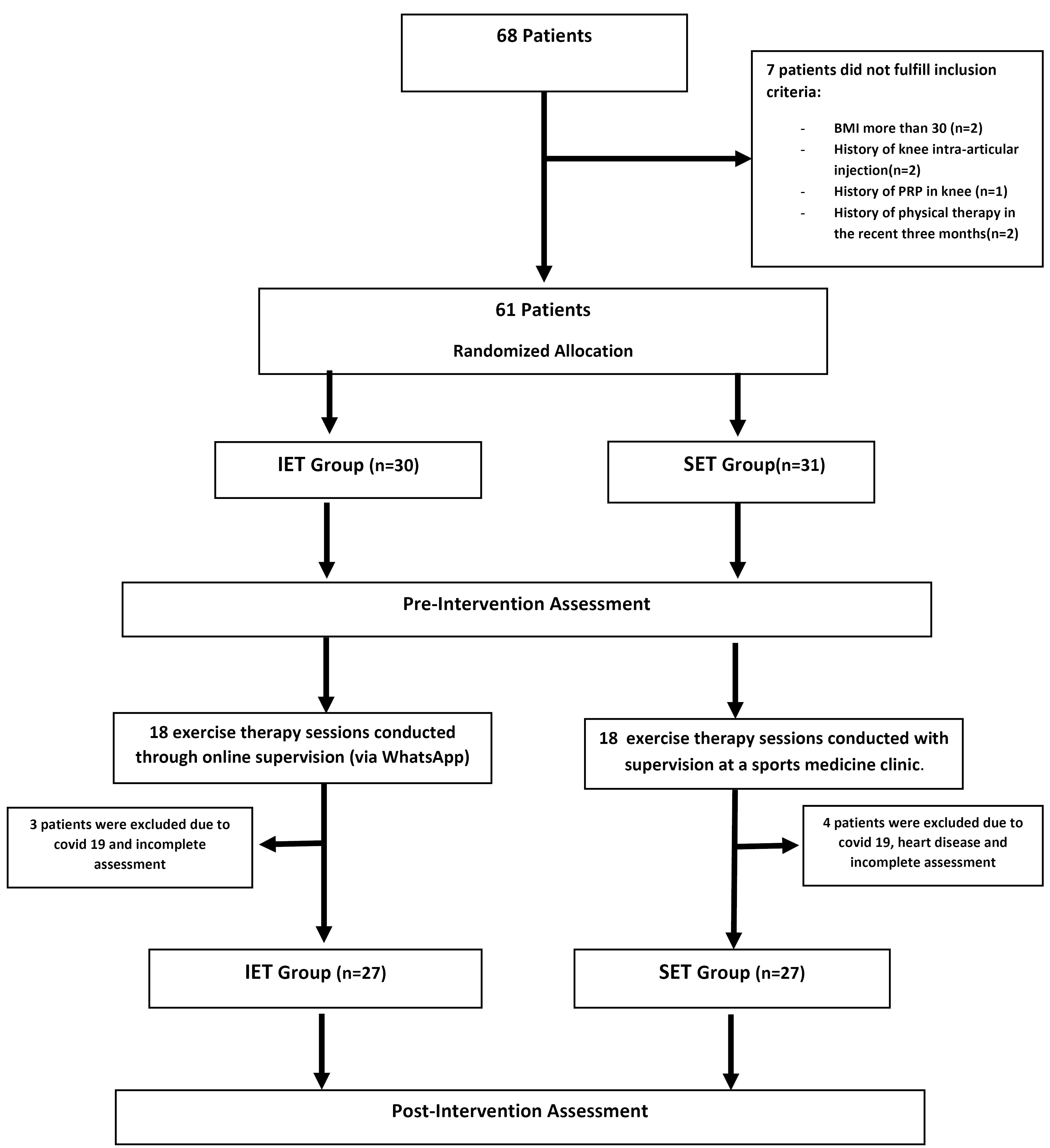
Figure 1.
Flow diagram of recruitment and allocation of the participants
.
Flow diagram of recruitment and allocation of the participants
Before their participation, all registered patients in the project signed a detailed informed consent form. Participants maintained the right to exit the study at any moment without any commitments. Furthermore, all participants were guaranteed the confidential and secure handling of their personal information.
Interventions
Each patient participated in 18 supervised sessions, conducted three times a week. The exercise program followed a progressively similar plan, carried out three times a week for 6 weeks for both groups. It encompassed 14 exercises (as detailed in Table 1) and included a 10-minute warm-up and cool-down parts involving walking and stretches for the lower limbs. The same expert carried out the interventions for both groups.
Table 1.
Detailed description of the exercise protocol for SET and IET groups (
Figure S1)
| # |
Exercise
|
First two weeks
|
Second two weeks
|
Third two weeks
|
| 1 |
Quadriceps static contraction |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Six sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 2 |
Straight legs raising (SLR) |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition |
Six sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 3 |
SLR in the sitting position with ankle dorsiflexion |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition |
Six sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 4 |
Terminal knee extension with a pillow below the knees in the supine position |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition |
Six sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 5 |
Static contraction of hip adductor with a pillow between two legs. |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition |
Six sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 6 |
Wall-sit at a 90-degree knee flexion angle |
One set of 10 repetitions in each
session with five second-hold. |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 7 |
Standing Leg Curl |
One set of 10 repetitions in each
session with five second-hold. |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 8 |
Sit to stand |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 9 |
Heel raising of both feet |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 10 |
Straight leg raises (SLR) with a proper weight cuff. |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 11 |
Mini Squat movement with isometric hip adduction |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 12 |
Terminal knee extension with TheraBand |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 13 |
The resisted exercise of the quadriceps in the sitting position with a proper weight cuff. |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
| 14 |
Standing Hip Abduction |
- |
Two sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
Four sets of 10 repetitions per session, with a hold of five seconds for every repetition. |
SET group: The control or SET group, executed the progressive exercise protocol within the sports medicine clinic while being directly supervised by a sports medicine assistant.
IET group: Initially, the availability of internet access and messaging applications on the mobile devices of patients in the intervention or IET group was verified. In this study, an exercise therapy manual was prepared for the IET group, complete with images illustrating exercise techniques. This manual was provided to them on the assessment day prior to the intervention, with a request for them to adhere to the exercise therapy protocol, similar to the other groups. Additionally, the researcher established an online group for the patients in the IET group through the WhatsApp application. This group contained essential details regarding KOA, the exercise therapy procedure, and general advice. The information was conveyed through easily understandable text, supplemented with images demonstrating how to perform the exercise protocol.
Additionally, concise video clips, illustrating exercise protocols, were created and delivered individually to each patient through WhatsApp. The patients could use video calls if they had any questions about the exercises. All participants in IET were under online supervision, ensuring they received enough verbal and visual instructions for their exercise regimens. Additionally, to ensure exercise adherence, the IET cohort received weekly phone calls over 6 weeks to motivate them to perform the exercises and address any challenges they faced. Participants were asked about their exercise routines, and their responses were recorded in customized logbooks, designed for every patient.
To ensure consistency in medication among participants, all patients were advised to stop using non-steroidal anti-inflammatory drugs one week before and throughout the intervention. They could use Acetaminophen, up to a maximum of 2 grams per day, only if they experienced pain.
Measures of outcomes
In cases where patients had issues in both knees, the knee exhibiting more severe symptoms was selected for the study. Pain intensity was evaluated using the VAS, ranging from 0 to 10. FROM was assessed using a goniometer, while thigh muscle atrophy was evaluated by measuring TG with an inelastic tape positioned 18 cm above the upper pole of the patella.25
Additionally, the patients' physical functions were evaluated using the TUG and 6MWT. Secondary measures involved evaluating patients' scores on the pain, function, and stiffness subscales of the Persian version of the WOMAC, a culturally validated questionnaire.26
Analysis of data
Statistical analyses were performed using SPSS 26.0 software from SPSS Inc. in Chicago, IL, USA. Data normality was checked with the Kolmogorov-Smirnov test, and Levene's test was used to assess variance homogeneity. Paired t-tests were utilized for comparisons within the groups, and the independent sample t-test was employed to detect significant differences in the data between the groups. The analysis of covariance (ANCOVA) test was, also, employed to explore how pre-test values influenced the study outcomes. The significance level was established at P ≤ 0.05.
To evaluate the within-test consistency of objective assessments, a pilot study was conducted with ten healthy individuals who underwent repeated measurements one week apart. Reliability was determined using intraclass correlation coefficients (ICCs) with a 95% confidence interval. The ICCs for the initial and follow-up measurements were 0.93 for TG, 0.95 for FROM, 0.91 for the 6MW test, and 0.90 for the TUG test.
Results
Figure 1 displays a CONSORT diagram that outlines the flow of participants at each phase of the trial. A total of 68 patients were screened during a general recruitment call, with 61 qualifying for inclusion in the study. Ultimately, the study and assessments were completed by 54 patients.
Baseline characteristics of patients
There were no notable differences in demographic variables between the groups prior to the study (see Table 2). This was established through an independent sample t-test, signifying that the groups were well-matched.
Table 2.
Demographic and clinical characteristics of the participants at baseline
|
|
SET group
(n=27)
|
IET group
(n=27)
|
P
value
(
P
≤0.05)
|
|
Numerical variables, Mean (SD)
|
| Age (year) |
59.22 (2.83) |
57.03 (5.30) |
0. 110* |
| BMI (kg/m2) |
27.58 (2.67) |
28.03 (3.32) |
0. 597* |
| History of KOA (years) |
6.07 (2.67) |
5.94 (2.75) |
0. 249* |
|
Categorical variables, No. (%)
|
| Kellgren and Lawrence radiological classification |
|
|
|
| Grade II |
15 (55) |
14 (52) |
0.253* |
| Grade III |
12 (45) |
13 (48) |
0.347* |
| Involved knee |
|
|
|
| Right |
12 (45) |
14 (52) |
0.622 * |
| Left |
15 (55) |
13 (48) |
0.412* |
| Affected joint (%) |
|
|
|
| Tibiofemoral (TFJ) |
10 (37) |
10 (37) |
0.123 * |
| Patellofemoral (PFJ) |
2 (7.5) |
7 (26) |
0.092 * |
| Combined (TFJ + PFJ) |
15 (55.5) |
10 (37) |
0.512 * |
*Non-significant difference
Furthermore, no significant differences were observed between the groups at the start of the study concerning clinical data, which includes VAS, ROM, TUG, TG, 6MWT, and WOMAC scores, as illustrated in Table 3.
Table 3.
Differences in VAS, ROM, TG, TUG, 6MWT, and total and subscales WOMAC scores between the groups
|
Variables
|
Groups
|
P
value
(P
≤0.05)
|
SET (n=27)
Mean (SD)
|
IET (n=27)
Mean (SD)
|
| Visual analog scale (:0-10) |
|
|
|
| Pre-exercise therapy |
4.96 (1.25) |
5.41 (1.15) |
0.663 |
| Post- exercise therapy |
3.77 (1.15) |
4.15 (0.97) |
0.384 |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Flexion range of motion (degree) |
|
|
|
| Pre-exercise therapy |
114.33 (5.76) |
115.32 (6.79) |
0.703 |
| Post- exercise therapy |
116.33 (5.58) |
117.50 (6.21) |
0.669 |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Thigh girth (cm) |
|
|
|
| Pre-exercise therapy |
53.70 (4.40) |
56.12 (2.63) |
0.120 |
| Post- exercise therapy |
54.30 (4.48) |
57.25 (3.11) |
0.437 |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Timed up and go test (second) |
|
|
|
| Pre-exercise therapy |
10.12 (1.78) |
8.98 (1.45) |
0.073 |
| Post- exercise therapy |
9.53 (1.76) |
7.42 (1.36) |
< 0.001* |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Six-minute walk test (meter) |
|
|
|
| Pre-exercise therapy |
403.36 (63.35) |
477.78 (45.85) |
0.086 |
| Post- exercise therapy |
473.59 (76.00) |
517.87 (52.38) |
< 0.017* |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Pain subscale in WOMAC |
|
|
|
| Pre-exercise therapy |
9.25 (0.75) |
9.37 (0.68) |
0.188 |
| Post- exercise therapy |
7.13 (0.68) |
7.19 (0.45) |
0.095 |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Stiffness subscale in WOMAC |
|
|
|
| Pre-exercise therapy |
3.64 (1.21) |
3.82 (1.63) |
0.697 |
| Post- exercise therapy |
2.84 (0.85) |
2.89 (0.42) |
0.498 |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Function subscale in WOMAC |
|
|
|
| Pre-exercise therapy |
32.78 (2.43) |
34.16 (2.96) |
0.638 |
| Post- exercise therapy |
26.86 (2.19) |
27.22 (2.37) |
0.231 |
|
P value |
< 0.0001* |
< 0.0001* |
|
| Total score in WOMAC |
|
|
|
| Pre-exercise therapy |
46.433 (3.82) |
47.86 (3.44) |
0.587 |
| Post- exercise therapy |
37.23 (3.22) |
38.95 (2.86) |
0.271 |
|
P value |
< 0.0001* |
< 0.0001* |
|
* Non-significant difference
Intragroup comparisons
Significant differences were found in TUG and 6MWT between the groups using an independent sample t-test (P ≤ 0.05). Additionally, significant differences were identified between the groups in other outcomes (see Table 3). This suggests that the SET and IET approaches yield similar results for VAS, TG, and FROM. However, the IET group shows a notable enhancement in functional test outcomes compared to the other group.
In this study, we applied ANCOVA, incorporating pre-test values as covariates. This approach helps manage the influence of pre-test scores as a carry-over effect. Also, this approach creates a framework that enables to study of the treatment effects distinct from the potential impact of the initial pre-test scores. We used G*Power 3.1 software to calculate the effect size and verified the assumptions of consistent regression slopes and homogeneity of variances for ANCOVA. When applying the ANCOVA statistical approach to compare the groups while accounting for pre-intervention measures as covariates, no statistically significant differences were detected in the outcomes following the intervention:
-
VAS (P = 0.8),
-
FROM (P = 0.38),
-
TG (P = 0.78),
-
TUG (P = 0.42),
-
6MWT (P = 0.11),
-
WOMAC pain subscale (P = 0.54),
-
WOMAC stiffness subscale (P = 0.36),
-
WOMAC function subscale (P = 0.39),
-
WOMAC total score (P = 0.87).
Discussion
This study focuses on the impact of two intervention approaches on variables such as pain, range of motion (ROM), and physical function of the patients with KOA. Through a comprehensive analysis of the trial's results, this discussion aims to provide insights into the potential advantages, limitations, and broader implications of both clinic-supervised and internet-based exercise therapies in managing KOA. This section sheds light on the observed differences, similarities, and underlying mechanisms, offering insights into the progress of therapeutic strategies aimed at improving patients' quality of life and well-being with this prevalent musculoskeletal condition. According to the results obtained from this study, both SET and IET in both groups demonstrated the capacity to diminish pain, enhance knee flexion range, ameliorate TG, and improve physical performance in women diagnosed with primary KOA. The impacts of exercise therapy were relatively consistent in both groups, regardless of the supervision method employed.
Pain
Alleviating pain in KOA patients is crucial, as it significantly impacts their functioning and quality of life. A key finding in this study was that both groups reported a decrease in knee pain after the exercise therapy. The lack of differences in pain outcomes immediately after the intervention among the groups may be due to the efficacy of exercise therapy in enhancing patients' conditions. Multiple analgesic mechanisms are likely involved in these outcomes, such as the release of endogenous opioids and non-opioids, exercise-induced hypoalgesia, and the anti-inflammatory effects of exercise, which contribute to reduced levels of inflammation biomarker.25,27,28 Thus, it seems that the observed reduction in pain may be attributed to the enhancements in muscle strength.
There was no statistically significant difference between the groups, whether under direct in-person clinic supervision or through online monitoring, suggesting a relatively comparable influence from both sets.
FROM
Patients suffering from KOA undergo pain and reduced physical involvement, resulting in the development of fibrosis in tissues around the joint and adaptive tightening of muscles. As a result, this limits the ROM in the knee. Our results indicate that there were not significant differences between the groups after the exercise therapy. Additionally, as knee KOA progresses, the ROM in the knee gradually declines. However, exercises promote greater flexibility in the muscles and surrounding soft tissues of the joint, leading to enhanced ROM for patients, irrespective of the monitoring method employed. Corroborating the present study's findings, Dighe and Dabholkar observed no enhancement in knee ROM when comparing tele-physiotherapy utilizing applications to exercise therapy conducted with clinic supervision.29 Unfortunately, the knee ROM has less been evaluated in knee OA-related studies.
Thigh girth
Measuring TG is a widely utilized technique for assessing the decrease in thigh muscle mass.25 A statistical difference in TG was noted between the pre- and post-exercise therapy periods in both groups. Moreover, there was no notable difference in TG between the two groups, likely because both followed the same exercise therapy protocol. This finding supports the idea that both supervision methods have an equivalent effect on exercise therapy for the groups. Unfortunately, no previous studies have examined the effects of clinic-supervised versus internet-supervised exercise therapy on TG in patients with KOA. The exercise protocol used for both groups positively influenced TG and improved the overall condition of the thigh muscles, regardless of the supervision method.
Functional tests
Functional disability in KOA patients often stems from pain, muscle weakness, and atrophy. Our results showed significant differences between both groups in the outcomes of the 6MW and TUG tests following the exercise therapy, with results favoring the IET group, unlike the other outcomes. However, it is important to note that although a significant difference was identified in functional tests using the independent samples t test, no significant difference was observed according to the ANCOVA statistical test.
This may be attributed to the ANCOVA analysis being impacted by the interdependence of the initial test values. Consequently, the statistical outcomes from other assessed variables were referenced, and the significant differences between the groups in functional tests were not taken into account. As a result, it is stated that the SET and IET groups are considered to be similar.
In a meta-analysis, Yang et al studied the differences between face-to-face exercise therapy and Internet-supervised exercise therapy. Similar to the findings of the present study; they detected no significant differences between these two methods concerning functional test results30. The outcomes from studies by Williams et al, Allen et al, and Xie et al, which explored the comparison of clinic-based SET and internet-based approaches, align with the results of our own research.20,31,32
Based on our findings, it appears that patients in the IET group exhibited a heightened focus on their exercise routines. This heightened commitment can be attributed to the appeal of mobile applications and the increased psychological motivation stemming from their participation in social media. Unlike SET, where patients primarily derive motivation from their therapists and the desire to manage their clinical symptoms, the IET group draws motivation from multiple sources. In addition to the aforementioned factors, they are influenced by peer feedback and the exchange of experiences with other Internet group patients. This collective sharing of opinions and experiences significantly enhances their motivation, resulting in a more determined effort to engage in therapeutic exercises. In essence, patients in the IET group appear to possess greater mental motivation to enhance their performance compared to those in the SET group.
Chen et al have determined that the adoption of technology/internet-supported exercise programs for treating KOA patients, is a highly beneficial and efficient approach to pain management, enhancing clinical symptoms, and improving patients' quality of life and function. It is anticipated that this approach will soon supersede conventional methods.33
Nevertheless, our study does possess several limitations. First, the sample size is constrained and mainly comprises non-obese female patients with KOA (grades 2 and 3). Consequently, the generalizability of the findings to other populations, such as male KOA patients, remains uncertain. The effectiveness of exercise therapy in KOA patients is also a well-established concept, however, the comparison between SET and IET approaches could be considered somewhat novel. Additionally, it's worth noting that our findings only pertain to the short-term effects of exercise therapy since we did not track patients over an extended duration. Therefore, there is a need for prospective trials with larger and more diverse participant groups, encompassing both genders and longer follow-up periods for knee OA patients to address these limitations.
It should be acknowledged that the majority of current exercise therapy protocols face challenges such as poor patient adherence and limited use, particularly among KOA patients. These challenges arise from factors such as socioeconomic constraints, personal convictions, concerns about movements, and pain exacerbation during rehabilitation. Consequently, there is a pressing, cost-effective need for IET customized to KOA patients' needs. This approach can assist healthcare professionals in better aligning their rehabilitation goals.
Study Highlights
What is current knowledge?
-
Knee osteoarthritis (KOA) is a common condition in older adults, managed effectively through exercise therapy, particularly under supervision. Recently, internet-based exercise programs have gained attention for their accessibility, though more direct comparisons with clinic-based approaches are needed.
What is new here?
-
This study compares supervised and internet-based exercise therapy in KOA patients, showing both are equally effective. It highlights that internet-based therapy may enhance certain functional outcomes and offers a validated, accessible protocol suitable for older populations, especially in resource-limited settings.
Conclusion
Our findings indicate that both clinic-supervised and IET produce similar outcomes in reducing pain, improving range of motion, increasing thigh girth, and enhancing physical function in patients with KOA. Furthermore, IET emerges as a cost-effective, convenient, effective, and personalized approach for individuals managing KOA.
Competing Interests
No competing interests to declare.
Ethical Approval
This study received ethical approval from the Medical Ethics Committee of Iran University of Medical Sciences, assigned the code IR.IUMS.FMD.REC.1399.628, in compliance with the most recent version of the Helsinki Declaration. Furthermore, our study has been registered in the Iranian Registry of Clinical Trials with the ID IRCT20101228005486N8.
Supplementary Files
Supplementary file contains Figure S1.
(pdf)
Acknowledgements
The authors wish to express their gratitude to the patients for their generous investment of time, consent, and outstanding cooperation. We also acknowledge the invaluable support and assistance received from the academic staff and members of the Sports and Exercise Medicine Clinic at Hazarat Rasoul Akram hospital.
References
- Primorac D, Molnar V, Rod E, Jeleč Ž, Čukelj F, Matišić V. Knee osteoarthritis: a review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes (Basel) 2020; 11(8):854. doi: 10.3390/genes11080854 [Crossref] [ Google Scholar]
- Moezy A, Aliyari Z, Kavand S. Buckling in the Iranian patients with knee osteoarthritis: its frequency and correlation with physical activities and falling. J Kerman Univ Med Sci 2019; 26(4):297-306. doi: 10.22062/jkmu.2019.89523 [Crossref] [ Google Scholar]
- Jaiswal A, Goswami K, Haldar P, Salve HR, Singh U. Prevalence of knee osteoarthritis, its determinants, and impact on the quality of life in elderly persons in rural Ballabgarh, Haryana. J Family Med Prim Care 2021; 10(1):354-60. doi: 10.4103/jfmpc.jfmpc_1477_20 [Crossref] [ Google Scholar]
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392(10159):1789-858. doi: 10.1016/s0140-6736(18)32279-7 [Crossref] [ Google Scholar]
- Shamsi M, Safari A, Soroush A, Safari Y. The survey of knee osteoarthritis in the population over age 50 visited in the health bus in Kermanshah, Iran. J Aging Res 2021; 2021:9809565. doi: 10.1155/2021/9809565 [Crossref] [ Google Scholar]
- Nazari A, Moezy A, Nejati P, Mazaherinezhad A. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: a randomized controlled trial with 12-week follow up. Lasers Med Sci 2019; 34(3):505-16. doi: 10.1007/s10103-018-2624-4 [Crossref] [ Google Scholar]
- Azma K, Rezasoltani Z, Rezaeimoghaddam F, Dadarkhah A, Mohsenolhosseini S. Efficacy of tele-rehabilitation compared with office-based physical therapy in patients with knee osteoarthritis: a randomized clinical trial. J Telemed Telecare 2018; 24(8):560-5. doi: 10.1177/1357633x17723368 [Crossref] [ Google Scholar]
- Ruhdorfer A, Wirth W, Eckstein F. Association of knee pain with a reduction in thigh muscle strength - a cross-sectional analysis including 4553 osteoarthritis initiative participants. Osteoarthritis Cartilage 2017; 25(5):658-66. doi: 10.1016/j.joca.2016.10.026 [Crossref] [ Google Scholar]
- Rice DA, McNair PJ, Lewis GN. Mechanisms of quadriceps muscle weakness in knee joint osteoarthritis: the effects of prolonged vibration on torque and muscle activation in osteoarthritic and healthy control subjects. Arthritis Res Ther 2011; 13(5):R151. doi: 10.1186/ar3467 [Crossref] [ Google Scholar]
- Suzuki Y, Iijima H, Nakamura M, Aoyama T. Rate of force development in the quadriceps of individuals with severe knee osteoarthritis: a preliminary cross-sectional study. PLoS One 2022; 17(1):e0262508. doi: 10.1371/journal.pone.0262508 [Crossref] [ Google Scholar]
- Fransen M, McConnell S, Harmer AR, van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med 2015; 49(24):1554-7. doi: 10.1136/bjsports-2015-095424 [Crossref] [ Google Scholar]
- Sharma L. Osteoarthritis of the knee. N Engl J Med 2021; 384(1):51-9. doi: 10.1056/NEJMcp1903768 [Crossref] [ Google Scholar]
- Kong H, Wang XQ, Zhang XA. Exercise for osteoarthritis: a literature review of pathology and mechanism. Front Aging Neurosci 2022; 14:854026. doi: 10.3389/fnagi.2022.854026 [Crossref] [ Google Scholar]
- Brophy RH, Fillingham YA. AAOS clinical practice guideline summary: management of osteoarthritis of the knee (nonarthroplasty), third edition. J Am Acad Orthop Surg 2022; 30(9):e721-9. doi: 10.5435/jaaos-d-21-01233 [Crossref] [ Google Scholar]
- Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, Del Coso J, Leyton-Román M, Luque-Casado A. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: an umbrella review. Int J Environ Res Public Health 2021; 18(4):2023. doi: 10.3390/ijerph18042023 [Crossref] [ Google Scholar]
- Deyle GD, Allison SC, Matekel RL, Ryder MG, Stang JM, Gohdes DD. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther 2005; 85(12):1301-17. [ Google Scholar]
- Lim WB, Al-Dadah O. Conservative treatment of knee osteoarthritis: a review of the literature. World J Orthop 2022; 13(3):212-29. doi: 10.5312/wjo.v13.i3.212 [Crossref] [ Google Scholar]
- Bozgeyik S, Kinikli GI, Topal Y, Beydagi MG, Turhan E, Kilinç HE. Supervised exercises have superior effects compared to home-based exercises for patients with knee osteoarthritis following platelet-rich plasma injection. Res Sports Med 2024; 32(2):279-89. doi: 10.1080/15438627.2022.2102920 [Crossref] [ Google Scholar]
- Anwer S, Alghadir A, Brismée JM. Effect of home exercise program in patients with knee osteoarthritis: a systematic review and meta-analysis. J Geriatr Phys Ther 2016; 39(1):38-48. doi: 10.1519/jpt.0000000000000045 [Crossref] [ Google Scholar]
- Allen KD, Arbeeva L, Callahan LF, Golightly YM, Goode AP, Heiderscheit BC. Physical therapy vs internet-based exercise training for patients with knee osteoarthritis: results of a randomized controlled trial. Osteoarthritis Cartilage 2018; 26(3):383-96. doi: 10.1016/j.joca.2017.12.008 [Crossref] [ Google Scholar]
- Moezy A, Masoudi S, Nazari A, Abasi A. A controlled randomized trial with a 12-week follow-up investigating the effects of medium-frequency neuromuscular electrical stimulation on pain, VMO thickness, and functionality in patients with knee osteoarthritis. BMC Musculoskelet Disord 2024; 25(1):158. doi: 10.1186/s12891-024-07266-8 [Crossref] [ Google Scholar]
- Cottrell MA, Galea OA, O'Leary SP, Hill AJ, Russell TG. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehabil 2017; 31(5):625-38. doi: 10.1177/0269215516645148 [Crossref] [ Google Scholar]
- Najafi F, Darbandi M, Kazemi Neya S, Tokazebani Belasi M, Izadi N, Pasdar Y. Epidemiology of musculoskeletal disorders among iranian adults: results from a non-communicable disease cohort study. BMC Musculoskelet Disord 2023; 24(1):315. doi: 10.1186/s12891-023-06435-5 [Crossref] [ Google Scholar]
- Tore NG, Oskay D, Haznedaroglu S. The quality of physiotherapy and rehabilitation program and the effect of telerehabilitation on patients with knee osteoarthritis. Clin Rheumatol 2023; 42(3):903-15. doi: 10.1007/s10067-022-06417-3 [Crossref] [ Google Scholar]
- Moezy A, Kavand S, Angoorani H, Nazari A, Masoudi S. A randomized controlled trial of two exercise protocols on pain, function, and vastus medialis thickness in women with knee osteoarthritis. J Pain Manag 2021; 14(2):133-44. [ Google Scholar]
- Eftekhar-Sadat B, Niknejad-Hosseyni SH, Babaei-Ghazani A, Toopchizadeh V, Sadeghi H. Reliability and validity of Persian version of Western Ontario and McMaster Universities Osteoarthritis Index in knee osteoarthritis. J Anal Res Clin Med 2015; 3(3):170-7. doi: 10.15171/jarcm.2015.027 [Crossref] [ Google Scholar]
- Imoto AM, Peccin MS, Trevisani VF. Quadriceps strengthening exercises are effective in improving pain, function and quality of life in patients with osteoarthritis of the knee. Acta Ortop Bras 2012; 20(3):174-9. doi: 10.1590/s1413-78522012000300008 [Crossref] [ Google Scholar]
- Koltyn KF, Brellenthin AG, Cook DB, Sehgal N, Hillard C. Mechanisms of exercise-induced hypoalgesia. J Pain 2014; 15(12):1294-304. doi: 10.1016/j.jpain.2014.09.006 [Crossref] [ Google Scholar]
- Dighe P, Dabholkar T. Comparison of efficacy of telephysiotherapy with supervised exercise programme in management of patients suffering with grade I and II osteoarthritis. Journal of Exercise Science & Physiotherapy 2020; 16(1):30-9. doi: 10.18376/jesp/2020/v16/i1/154131 [Crossref] [ Google Scholar]
- Yang Y, Li S, Cai Y, Zhang Q, Ge P, Shang S. Effectiveness of telehealth‐based exercise interventions on pain, physical function and quality of life in patients with knee osteoarthritis: a meta‐analysis. J Clin Nurs 2023; 32(11-12):2505-20. doi: 10.1111/jocn.16388 [Crossref] [ Google Scholar]
- Williams QI, Gunn AH, Beaulieu JE, Benas BC, Buley B, Callahan LF. Physical therapy vs internet-based exercise training (PATH-IN) for patients with knee osteoarthritis: study protocol of a randomized controlled trial. BMC Musculoskelet Disord 2015; 16:264. doi: 10.1186/s12891-015-0725-9 [Crossref] [ Google Scholar]
- Xie SH, Wang Q, Wang LQ, Wang L, Song KP, He CQ. Effect of internet-based rehabilitation programs on improvement of pain and physical function in patients with knee osteoarthritis: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res 2021; 23(1):e21542. doi: 10.2196/21542 [Crossref] [ Google Scholar]
- Chen H, Zheng X, Huang H, Liu C, Wan Q, Shang S. The effects of a home-based exercise intervention on elderly patients with knee osteoarthritis: a quasi-experimental study. BMC Musculoskelet Disord 2019; 20(1):160. doi: 10.1186/s12891-019-2521-4 [Crossref] [ Google Scholar]