J Res Clin Med. 13:34591.
doi: 10.34172/jrcm.025.34591
Case Report
Heart on the right side: A rare case report of dextrocardia with situs solitus, L-TGA (levo-transposition of the great arteries) and single ventricle physiology
Gurusha Bahl Conceptualization, Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing, 1 
Md Sadique Hussain Data curation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing, 2, *
Dinesh K Upadhyay Formal analysis, Resources, 3
Narendra Meena Conceptualization, Methodology, Project administration, Validation, Visualization, Writing – original draft, 4
Rajveer Singh Formal analysis, Resources, 3
Tekchand Narang Investigation, Resources, Writing – original draft, 3
Author information:
1Department of Pharmacology, Jaipur National University Institute of Medical Science and Research Centre, Jaipur 302017, Rajasthan, India
2Uttaranchal Institute of Pharmaceutical Sciences, Uttaranchal University, Dehradun, 248007, Uttarakhand, India
3Department of Pharmacology, School of Pharmaceutical Sciences, Jaipur National University, Jaipur, 302017, Rajasthan, India
4Department of Medicine, Jaipur National University Institute for Medical Sciences and Research Center, Jaipur, 302017, Rajasthan, India
Abstract
Dextrocardia is a rare congenital anomaly characterized by the positioning of the heart towards the right side of the chest. The prevalence of dextrocardia with situs solitus is 1 in 30000 live births and 1 in 900000 in the adult population. We report the case of a 20-year-old male who presented with fever, shortness of breath, and an episode of epistaxis. He was found to have dengue IgM and Scrub typhus antibody positivity along with low hemoglobin, platelets, and total leucocyte count. Imaging studies revealed dextrocardia with situs solitus, single ventricle physiology, levo-transposition of great arteries (L-TGA), and moderate pulmonary stenosis. This case focuses on the importance of recognizing congenital heart diseases (CHDs) in patients with dextrocardia along with situs solitus. The patient had associated CHD with L-TGA, which is an uncommon type of CHD so this case report highlights the importance of careful evaluation of patients with suspected CHD and emphasizes the need for multidisciplinary management for the best outcomes.
Keywords: Dextrocardia, L-TGA, Pulmonary stenosis, Single ventricle physiology, Situs solitus
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
None.
Introduction
Dextrocardia can be defined as the embryologic development of the heart towards the right side so most of the heart’s bulk is positioned in the right hemithorax. Situs refers to the arrangement of the visceral organs and atria, which can be classified into: situs solitus which is normal visceroatrial arrangement, situs inversus which is a mirror image of the visceroatrial arrangement and situs ambiguous which is visceroatrial isomerism.1 Dextrocardia can be associated with situs solitus or situs inversus. The prevalence of dextrocardia with situs solitus is 1 in 30 000 live births and 1 in 900 000 in the adult population, while the prevalence of situs inversus in the adult population is 1 in 10 000.2 Situs solitus is defined as the right superior vena cava and right inferior vena cava connecting on the right side of the heart to the systemic right atrium, with a left-sided stomach and right-sided liver.3,4 Dextrocardia is mainly classified as per two considerations: (1) Types of the cardiac cycle which indicates the positions of the ventricles which is according to the association between the great arteries and (2) Type of viscera-atria situs which is the locations of the atria and viscera. Van Praagh et al described the different types of dextrocardia and classified them into three general types: solitus (normal or ordinary), inversus (mirror image of solitus), and abnormally symmetric viscera with asplenia.5 In this report, we present a case of 20 years old male with dextrocardia associated with situs solitus, single ventricle physiology, and levo-transposition of great arteries (L-TGA).
Case Presentation
A 20-year-old patient was admitted to the male medicine ward with chief complaints of fever, generalized weakness, body pain, shortness of breath, and an episode of epistaxis. A pan systolic murmur was heard radiating to the axilla and carotid, which was loud in the tricuspid area and II intercostal space (ICS) on the left side. On examination, his vital signs were BP 90/56 mm Hg and PR 84/min. He had low hemoglobin of 8.6 mg/dL, low total leucocyte count of 2630 cumm, and a low platelet count of 1.18 lacs/cumm. A chest X-ray indicated a right-sided ventricular shade with the cardiac apex oriented right side and pronounced bronchovascular marks, as depicted in Figures 1a and 1b. High-resolution computed tomography reports the impression of transposition of great vessels, grossly dilated main pulmonary artery, and hypoplastic aorta along with ground glass haziness (alveolar opacity) with hepatosplenomegaly suggestive of pulmonary edema due to pulmonary hypertension/anemia. Contrast-enhanced computed tomography scan of the whole abdomen examination as seen in Figure 2 revealed enlarged liver (22 cm), an enlarged spleen (18 cm) indicating hepatomegaly with mild ascites, splenomegaly, and mild right nephromegaly. Dengue IgM was reactive indicating dengue and scrub typhus antibody was found to be positive. Transthoracic echocardiography reported critical congenital heart disease (CCHD), dextrocardia with situs solitus, single ventricle physiology, L-TGA, moderate to severe regurgitation of the left AV valve, a left-sided aortic arch, and moderate pulmonary stenosis with the aorta located anterior to the dilated pulmonary artery and the left atrium being dilated as shown in Figures 3a and 3b. Further laboratory investigations revealed is discussed in Table 1.
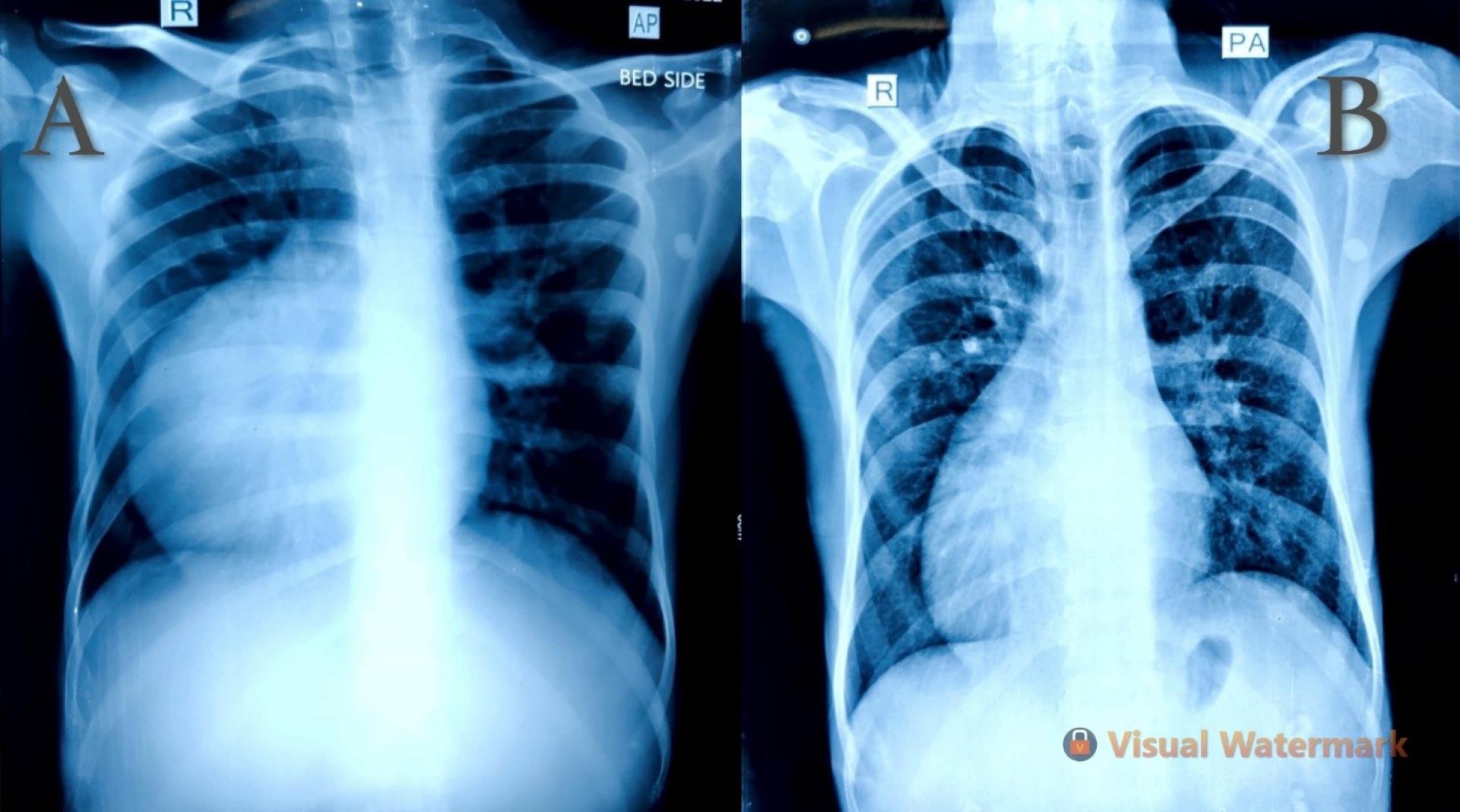
Figure 1.
(a) Anteroposterior chest X-ray confirming right-sided cardiac shadow with the cardiac apex pointing right side along with prominent broncho vascular markings, (b) X-ray chest posteroanterior showing dextrocardia
.
(a) Anteroposterior chest X-ray confirming right-sided cardiac shadow with the cardiac apex pointing right side along with prominent broncho vascular markings, (b) X-ray chest posteroanterior showing dextrocardia
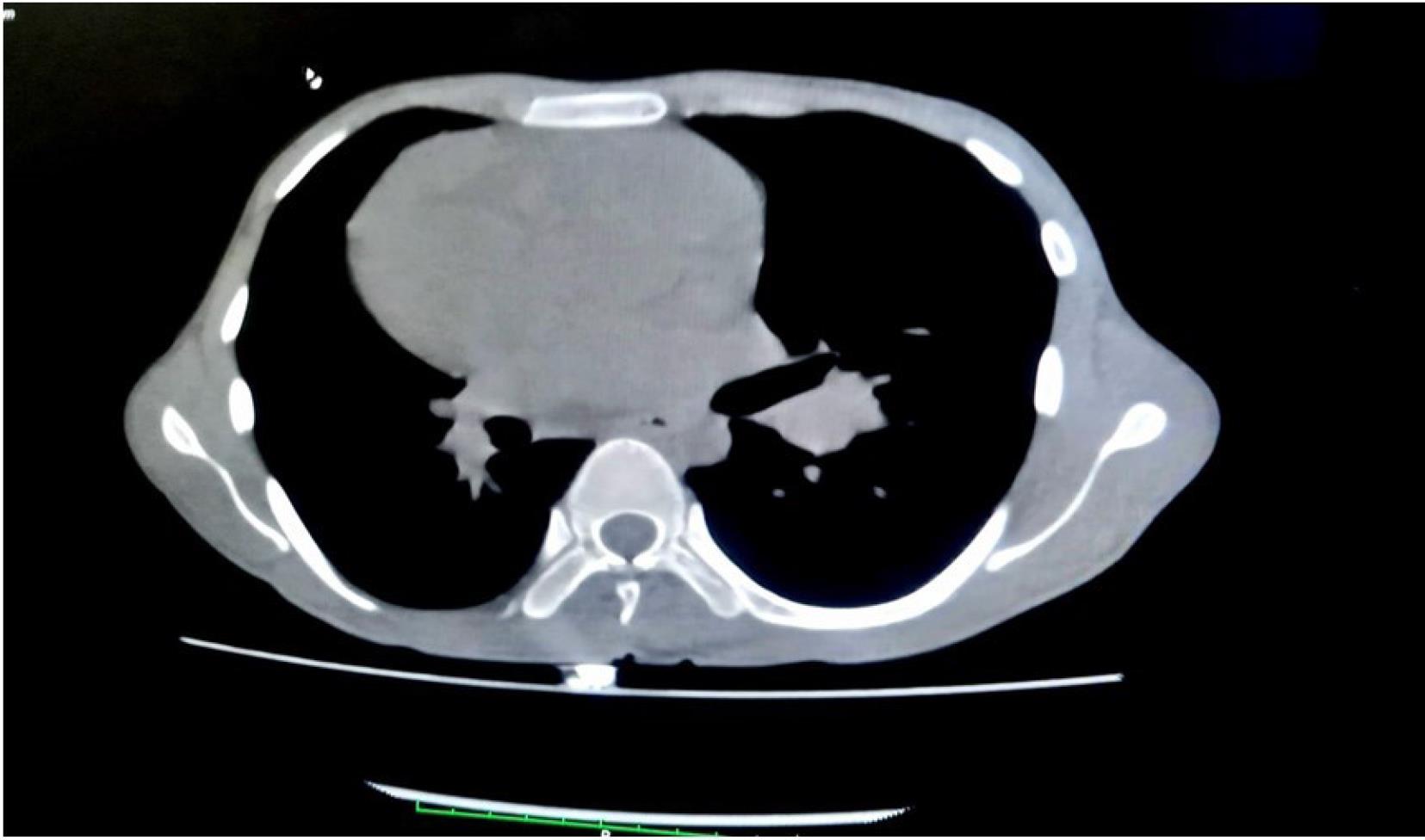
Figure 2.
Computed tomography shows an enlarged liver and spleen
.
Computed tomography shows an enlarged liver and spleen
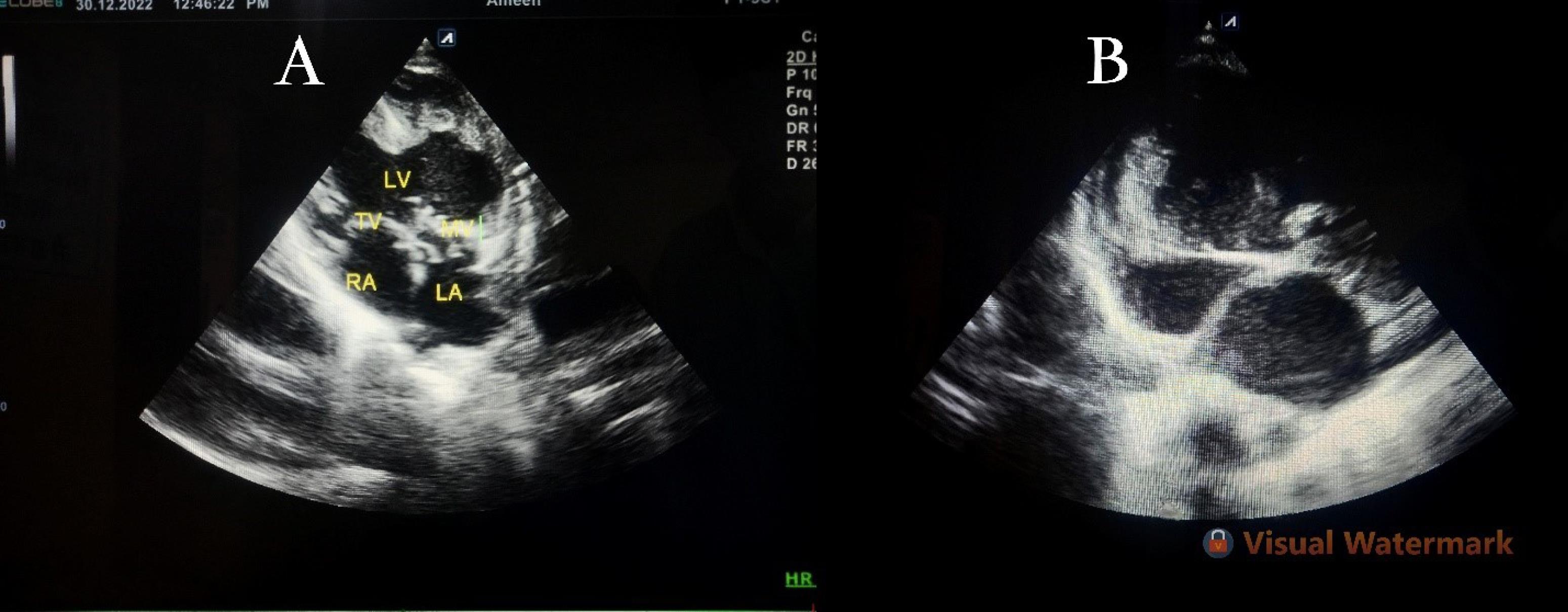
Figure 3.
(a) and (b): 2D-echo revealed dextrocardia, situs solitus with single ventricle physiology along with a dilated left atrium
.
(a) and (b): 2D-echo revealed dextrocardia, situs solitus with single ventricle physiology along with a dilated left atrium
Table 1.
Laboratory investigations of patient
|
Investigations
|
Results
|
Reference range
|
| Iron |
55.7 μg/dL (L) |
60–170 μg/dL |
| TIBC |
194.04 μg/dL (L) |
240–450 μg/dL |
| LDH (serum) |
1140 U/L(H) |
140–280 U/L |
| Serum total protein |
6.1 g/dL (L) |
6.4 – 8.3 g/dL |
| Serum albumin |
2.3 g/dl (L) |
3.8 - 4.4 g/dL |
| Serum globulin |
3.8 g/dl (H) |
2.3 – 3.6 g/dL |
| Sodium |
127.7 mmol/L (L) |
135-145 mmol/L |
L, low; H, High; TIBC, Total Iron-Binding Capacity
The rest of other parameters reported were normal. For the management of symptoms, the patient was given intravenous fluid normal saline 80 per hour along with IV amikacin 250 mg and IV piperacillin/tazobactam 2.25 g.
Discussion
Dextrocardia refers to the abnormal location of the heart, characterized by the ventricular apex being located in the right hemithorax (RH). In dextrocardia, the anatomical configuration of the organs of the abdomen may be classified as being typical (situs solitus) in 32%–35% of instances, flipped (situs inversus) in 35%–39%, and undetermined (situs ambiguous or isomerism) in 26%–28%. However, the atrial situs consistently aligns with the visceral situs.6 The human embryonic heart originates from a basic ventricular conduit that may loop to the left, creating an L-loop (levo), or to the right, resulting in a D-loop (dextro).7 Dextrocardia may arise from a D-bulboventricular looping that does not expand into the left hemithorax (LH) or from an L-bulboventricular loop that has successfully shifted apically into the RH. Separated dextrocardia with situs solitus, in-line great arteries, and D-loop ventricles may arise from the inadequate final leftward displacement of the ventricular apex during embryonic growth, as well as the inability to rotate into the LH, instead of from atypical motion of the apex into the RH. Notwithstanding the atypical positioning of the ventricles, the atria and abdominal organs retain their situs solitus.8 In most cases, situs solitus is associated with CHD accounting for incidence close to 100% according to a previous study by Garg et al.9 Echocardiography facilitates the precise non-intrusive identification of congenital cardiac anomalies, including CCHD and problems linked to dextrocardia.10 Solitary dextrocardia with situs solitus has a right-sided cardiac apex, with the morphologic left atrium positioned to the left of the morphologic right atrium; the right lung contains 3 lobes, while the left lung has only two. The stomach and spleen are situated on the left along with the larger lobe of the liver on the right. The treatment of dextrocardia is supportive and symptomatic according to the need but if the condition involves other more serious cardiac malformations treatment varies accordingly.6
Conclusion
We presented a case of a 20-year-old male with dextrocardia associated with situs solitus, single ventricle physiology, and L-TGA. This case report talks about the importance of recognizing CHDs in patients with dextrocardia along with situs solitus and the need for a significant comprehensive clinical and laboratory evaluation in such cases. Our patient had associated CHD with L-TGA, so this case report highlights the importance of careful evaluation of patients with suspected CHD and emphasizes the need for multidisciplinary management for the best outcomes. Early diagnosis and management can improve the patient’s prognosis and quality of life.
Competing Interests
None.
Ethical Approval
Written informed consent was obtained from the patient for publication of this case report including the clinical information and accompanying images. Also, the patient was assured that his name and initials will not be published.
Acknowledgements
We take this opportunity to thank all the authors and faculty members for their continuous support and guidance to publish this case report.
References
- Reidy JF. The chest radiograph. In: Anderson RH, Baker EJ, MaCartney FJ, Rigby ML, Shinebourne EA, Tynan M, eds. Paediatric Cardiology. London: Churchill Livingstone; 2002. p. 285-93.
- McCaskie AW, Thompson MM, Underwood MJ, Pallot DJ. A case of dextrocardia with normal situs. Acta Anat (Basel) 1991; 142(4):288-92. doi: 10.1159/000147204 [Crossref] [ Google Scholar]
- Bohun CM, Potts JE, Casey BM, Sandor GG. A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol 2007; 100(2):305-9. doi: 10.1016/j.amjcard.2007.02.095 [Crossref] [ Google Scholar]
- Offen S, Jackson D, Canniffe C, Choudhary P, Celermajer DS. Dextrocardia in adults with congenital heart disease. Heart Lung Circ 2016; 25(4):352-7. doi: 10.1016/j.hlc.2015.09.003 [Crossref] [ Google Scholar]
- Van Praagh R, Van Praagh S, Vlad P, Keith JD. Anatomic types of congenital dextrocardia: diagnostic and embryologic implications. Am J Cardiol 1964; 13:510-31. doi: 10.1016/0002-9149(64)90159-6 [Crossref] [ Google Scholar]
- Srikant S, Dave D, Dave D. Isolated dextrocardia with situs solitus - dextroversion in a Ugandan baby: a case report. Int Med Case Rep J 2021; 14:797-800. doi: 10.2147/imcrj.S340185 [Crossref] [ Google Scholar]
- Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics 1999; 19(4):837-52; discussion 53. doi: 10.1148/radiographics.19.4.g99jl31837 [Crossref] [ Google Scholar]
- Elliott LP, Jue KL, Amplatz K. A roentgen classification of cardiac malpositions. Invest Radiol 1966; 1(1):17-28. doi: 10.1097/00004424-196601000-00025 [Crossref] [ Google Scholar]
- Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N. Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol 2003; 88(2-3):143-55. doi: 10.1016/s0167-5273(02)00539-9 [Crossref] [ Google Scholar]
- Huhta JC, Hagler DJ, Seward JB, Tajik AJ, Julsrud PR, Ritter DG. Two-dimensional echocardiographic assessment of dextrocardia: a segmental approach. Am J Cardiol 1982; 50(6):1351-60. doi: 10.1016/0002-9149(82)90474-x [Crossref] [ Google Scholar]