J Res Clin Med. 13:34583.
doi: 10.34172/jrcm.025.34583
Case Report
Sphenoethmoid mucocele: a rare cause of optic neuropathy
Witoon Mitarnun Conceptualization, Data curation, Formal analysis, Investigation, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, * 
Korrapat Aegakkatajit Conceptualization, Data curation, Formal analysis, Investigation, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, 2
Nutdanai Roila Conceptualization, Data curation, Formal analysis, Investigation, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, 3
Nithinan Uepechpong Conceptualization, Data curation, Formal analysis, Investigation, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, 4
Author information:
1Department of Internal Medicine, Buriram Hospital, Buriram, Thailand
2Department of Otolaryngology, Buriram Hospital, Buriram, Thailand
3Department of Internal Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
4Department of Pathology, Buriram Hospital, Buriram, Thailand
Abstract
Introduction:
The causes of optic neuropathy include ischemic optic neuropathy, infectious agents, inflammatory processes, and compressive lesions. Although a paranasal sinus mucocele is a rare cause of compressive optic neuropathy, it can be treatable with early diagnosis and appropriate management. This study aims to highlight the importance of recognizing and managing paranasal sinus mucoceles as a treatable cause of optic neuropathy.
Case Report:
A 61-year-old woman with diabetes mellitus and dyslipidemia who presented with a one-month history of vision loss in her left eye. Magnetic resonance imaging revealed a cystic lesion compressing the left optic nerve, suggestive of a sphenoethmoid mucocele. Mucocele marsupialization and antibiotics improved her vision, highlighting the paranasal sinus mucocele as a potential cause of optic neuropathy.
Conclusion:
Recognizing paranasal sinus mucoceles as a potential cause of optic neuropathy is important, despite their rarity, as they may be treatable. A multidisciplinary approach, including surgical intervention and infection control, is key to their management.
Keywords: Cystic lesion, Endoscopic sinus surgery, Mucocele, Optic neuropathy, Sphenoethmoid mucocele
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
No funding was received for this study.
Introduction
Optic neuropathy is characterized by damage or dysfunction of the optic nerve, which can result in vision loss or impairment. Various etiological factors contribute to optic neuropathy, including ischemic optic neuropathy, infectious agents, inflammatory processes, and compressive lesions.1 Liu et al. discovered that pituitary adenoma (35%), meningioma (17%), and aneurysm (13%) were frequent causes of compressive optic neuropathy.2 Additionally, they observed a notable correlation between the duration until treatment and the degree of visual field improvement.2
Paranasal sinus mucoceles are one of the less common causes of compressive optic neuropathy.3-5 They are cystic lesions lined with epithelium and filled with mucus, which develop due to the blockage of sinus ostia. This blockage can occur due to various factors such as chronic inflammation, infection, polyps, or prior sinus surgery. As mucus accumulates within the sinus, it could lead to cyst enlargement and erosion of the sinus bony wall.5 They are typically located in the frontal and ethmoid sinuses. The common symptom of paranasal sinus mucoceles is nasal congestion. Additional manifestations might include facial pain and headaches. If they expand and press on adjacent tissues, patients may encounter vision issues or neurological symptoms.
In the context of this report, we present a rare case of compressive optic neuropathy due to a sphenoethmoid mucocele, which exhibited clinical improvement after treatment.
Case Report
A 61-year-old woman with diabetes mellitus and dyslipidemia, who was taking medication including metformin (2000 mg/d), glipizide (20 mg/d), and simvastatin (10 mg/d), presented at Buriram hospital, a government regional hospital located in Buriram province, Thailand, with a one-month history of painless, progressive vision loss in her left eye. Before this visit, she had been to the private clinic several times regarding her condition, but no definitive diagnosis had been made. The patient’s vision problem persisted and progressed further. She had previously been diagnosed and treated for COVID-19 at another hospital, presenting with mild upper respiratory infection symptoms three weeks before the onset of visual symptoms in the left eye. Other aspects of her medical history were not significant. She denied any prior visual problems.
At the outpatient department, an ophthalmologist conducted an examination, demonstrating a relative afferent pupillary defect (RAPD) in the left eye. Her best-corrected visual acuity was 20/20in the right eye and hand motion in the left eye. Fundoscopic examination revealed no disc swelling. Other neurological examinations, including other cranial nerve assessments, motor function tests, sensory examination tests, and cerebellar function tests, as well as the general physical examinations, including cardiovascular, respiratory, and abdominal assessments, were unremarkable. An ophthalmologist initially suspected non-arteritic ischemic optic neuropathy (NAION), considering diabetes mellitus as a predisposing factor. However, other causes of optic neuropathy could not be ruled out. Subsequently, the ophthalmologist consulted the neurologist to admit the patient to the department of internal medicine for further investigations.
The blood analysis, including the complete blood count, along with assessments of kidney and liver function, revealed no concerning abnormalities. Her fasting blood sugar was 171.8 mg /dL, with a hemoglobin A1c level of 10.8%. Her cholesterol level was 160.3 mg /dL, with a low-density lipoprotein level of 86 mg /dL. Serology tests for human immunodeficiency virus and hepatitis B and C virus, as well as the Venereal Disease Research Laboratory test, all yielded negative results. Magnetic resonance imaging (MRI) of the orbit with gadolinium revealed a well-defined cystic lesion (measuring 2.8 cm × 2.2 cm × 1.9 cm) in the left sphenoethmoid sinus, accompanied by adjacent bone destruction and compression of the left optic nerve (see Figure 1).
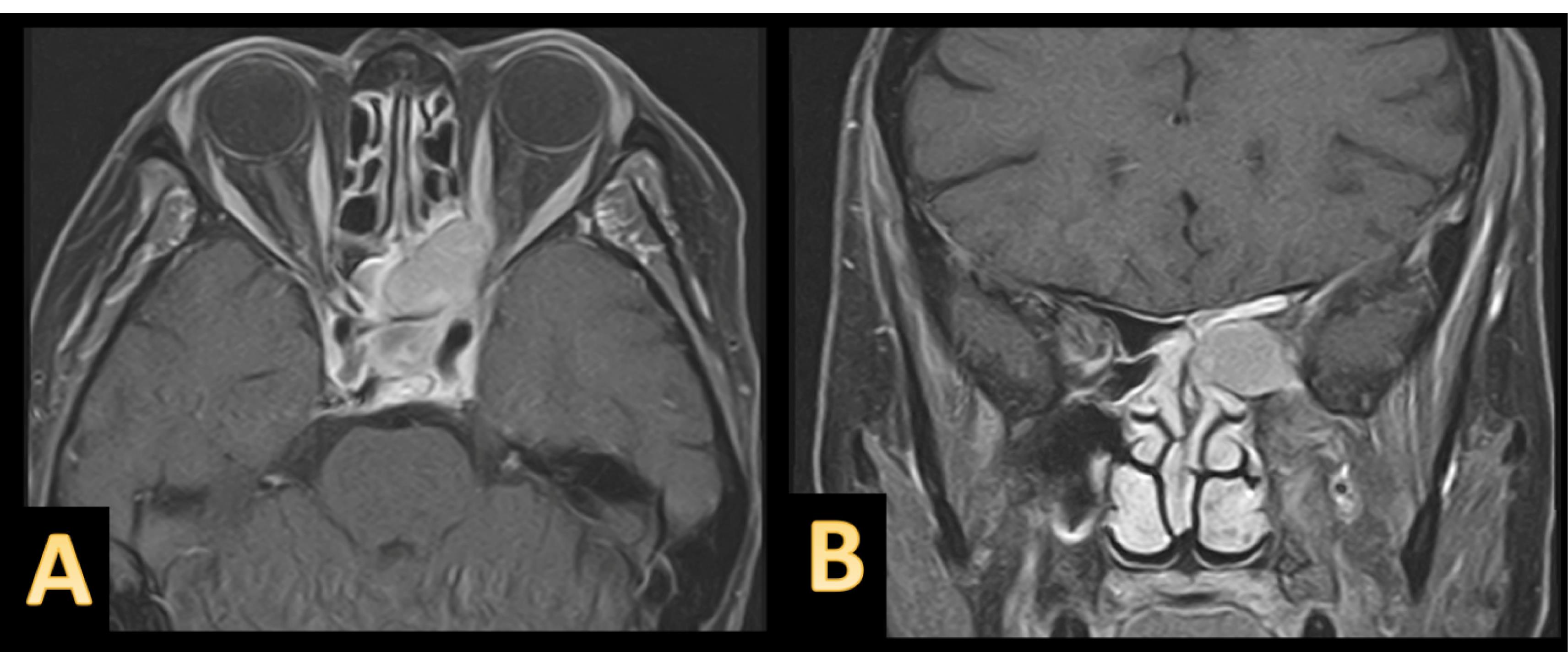
Figure 1.
subtitle:Gadolinium-Enhanced Orbital MRI of a Patient with Sphenoethmoid Mucocele. Axial (A) and coronal (B) gadolinium-enhanced orbital MRI revealed a well-defined cystic lesion without gadolinium enhancement in the left sphenoid sinus extending to the left ethmoid sinus, with adjacent bone destruction and compression of the left optic nerve, consistent with a sphenoethmoid mucocele
.
subtitle:Gadolinium-Enhanced Orbital MRI of a Patient with Sphenoethmoid Mucocele. Axial (A) and coronal (B) gadolinium-enhanced orbital MRI revealed a well-defined cystic lesion without gadolinium enhancement in the left sphenoid sinus extending to the left ethmoid sinus, with adjacent bone destruction and compression of the left optic nerve, consistent with a sphenoethmoid mucocele
Therefore, an otolaryngology consultation was promptly requested. The endonasal endoscopic surgery, with ethmoidectomy and a large sphenoidotomy to marsupialize the lesion, was performed the following day without any intraoperative or postoperative complications. Intraoperative findings included clear, yellow fluid in the cystic lesion. By histopathological evaluation of the cyst wall tissue, a pathologist confirmed the diagnosis of mucocele. Post-operation, she received oral amoxicillin/clavulanate (amoxicillin 1,750 mg/d and clavulanate 250 mg/d) for one week to control the infection. One week post-operation, she experienced improved vision in her left eye, with the visual acuity in her left eye improving from hand motion to finger counting.
Discussion
The patient experienced painless vision loss in the left eye without swelling of the optic disc. Additionally, there was a positive RAPD in the left eye, leading to a diagnosis of optic neuropathy. In this case, the differential diagnosis of optic neuropathy includes post-COVID-19 optic neuritis, NAION, compressive optic neuropathy, and other potential causes.1,6 However, an orbit MRI with gadolinium revealed a distinct cystic lesion located in the left sphenoethmoid sinus, showing associated bone damage and compression of the left optic nerve, consistent with a paranasal sinus mucocele. Other potential differential diagnoses, apart from a paranasal sinus mucocele, encompass paranasal sinus tumors such as inverted papilloma or sinonasal carcinoma. However, most tumors typically exhibit enhancement with gadolinium contrast.7 Another feasible diagnosis is mucus retention cysts, but these usually do not entirely fill the sinus and typically do not cause any bony erosion.7 Nonetheless, our case was confirmed as a diagnosis of paranasal sinus mucocele based on pathological findings.
In our case, the cause of the sphenoethmoid mucocele might be attributed to a previous upper respiratory tract infection due to COVID-19, resulting in the blockage of sinus ostia and accumulation of mucus, subsequently leading to the development of a mucocele. The mucocele causes osteolysis through the action of prostaglandins and collagenases, resulting in bony destruction and subsequent damage to adjacent structures, including the optic nerve.5 The study by Kim et al. investigated ninety-six cases of paranasal sinus mucoceles in patients presenting with ophthalmologic symptoms.8 Periorbital swelling and pain were the most prevalent, occurring in 36.4% of the patients. Additionally, eighteen patients (18.8%) were diagnosed with optic neuropathy.8 Among these eighteen patients, ten experienced improvements in their vision following surgical intervention.8 The study also revealed that the presence of infection was the determining factor affecting postoperative visual outcomes.8 Therefore, in the present case, surgical drainage was performed, and infection was controlled using oral antibiotics, resulting in clinical improvement observed one week after surgery. Our findings highlight that both surgical intervention and the implementation of effective infection control are important strategies when managing mucoceles associated with optic neuropathy.
Conclusion
Although paranasal sinus mucoceles are indeed a rare cause of optic neuropathy, it is crucial to recognize them as a potential cause since they may be treatable. The management and diagnosis of paranasal sinus mucoceles necessitate a multidisciplinary approach, and surgical intervention along with effective infection control are key strategies in their treatment.
Competing Interests
No conflict of interest in this study.
Ethical Approval
The ethics committee of Buriram Hospital approved this study (IRB: BR 0033.102.1/23), and the patient provided informed consent.
Acknowledgements
We express our gratitude to the patient for her cooperation.
References
- Voss E, Raab P, Trebst C, Stangel M. Clinical approach to optic neuritis: pitfalls, red flags and differential diagnosis. Ther Adv Neurol Disord 2011; 4(2):123-34. doi: 10.1177/1756285611398702 [Crossref] [ Google Scholar]
- Liu A, Craver EC, Bhatti MT, Chen JJ. Population-based incidence and outcomes of compressive optic neuropathy. Am J Ophthalmol 2022; 236:130-5. doi: 10.1016/j.ajo.2021.10.018 [Crossref] [ Google Scholar]
- Che SA, Lee YW, Yoo YJ. Compressive optic neuropathy due to posterior ethmoid mucocele. BMC Ophthalmol 2023; 23(1):426. doi: 10.1186/s12886-023-03168-w [Crossref] [ Google Scholar]
- Oka K, Ando W, Hagiya H, Higaki T, Otsuka F. Rhinogenic optic neuropathy with hemianopia caused by ethmoidal sinus mucocele. Clin Case Rep 2022; 10(12):e6696. doi: 10.1002/ccr3.6696 [Crossref] [ Google Scholar]
- Capra GG, Carbone PN, Mullin DP. Paranasal sinus mucocele. Head Neck Pathol 2012; 6(3):369-72. doi: 10.1007/s12105-012-0359-2 [Crossref] [ Google Scholar]
- Mitarnun W, Naksanguan T, Laoharattanahirun N, Roekrat P, Kimavaha S, Kajornrith W. Myelin-oligodendrocyte glycoprotein antibody-associated optic neuritis following SARS-CoV-2 pneumonia: a case report. Neurol Clin Neurosci 2022; 10(3):181-2. doi: 10.1111/ncn3.12595 [Crossref] [ Google Scholar]
- Gaillard F, Tran M, Glick Y. Paranasal sinus mucocele. Radiopaedia.org. Available from: https://radiopaedia.org/articles/paranasal-sinus-mucocele-1?lang=us. Accessed August 29, 2023.
- Kim YS, Kim K, Lee JG, Yoon JH, Kim CH. Paranasal sinus mucoceles with ophthalmologic manifestations: a 17-year review of 96 cases. Am J Rhinol Allergy 2011; 25(4):272-5. doi: 10.2500/ajra.2011.25.3624 [Crossref] [ Google Scholar]