J Res Clin Med. 12:12.
doi: 10.34172/jrcm.34561
Original Article
A comparative investigation of therapeutic effects of rose and lavender aromatherapy on hemodynamic symptoms of recently diagnosed diabetic patients: A single-blind randomized cross-over controlled clinical trial
Pooneh Yousefi Conceptualization, Investigation, Methodology, Resources, Supervision, Visualization, 1 
Saeed Hosseini Teshnizi Conceptualization, Methodology, Resources, Visualization, 1
Aref Faghih Conceptualization, Investigation, Methodology, Resources, Visualization, 1
Mohammad Hossein Taklif Conceptualization, Investigation, Methodology, Resources, Supervision, Visualization, 2, *
Author information:
1Department of Nursing, Faculty of Nursing and Midwifery, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
2Student Research Committee, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
Abstract
Introduction:
Diabetes is a chronic and widespread problem with broad effects on human physiological systems, including significant impacts on hemodynamic symptoms, which can significantly affect the patient’s recovery process and quality of life. This study was conducted to compare the effects of rose and lavender aromatherapy on hemodynamic symptoms in patients with a recent diabetes diagnosis.
Methods:
In this cross-over controlled clinical trial study, three distinct groups were employed: two experimental groups (aromatherapy with rose and lavender) and a single control group. Pre-test and post-test assessments were conducted before and after the intervention on a total of 45 diabetic patients in 2022 at the Hormoz Clinic in Bandar Abbas. The interventions occurred over three sessions, with each patient receiving different treatments during different periods (first, second, and third stages). A one-week washout period was implemented between the stages to mitigate any potential carryover effects. Before initiating the interventions, demographic variable questionnaires and hemodynamic symptoms (systolic and diastolic blood pressure, and pulse rate) were documented both before and after the interventions. Data were analyzed using Stata version 14.0 and SPSS version 26 statistical software.
Results:
The mean diastolic blood pressure (P=0.459), systolic blood pressure (P=0.908), and pulse rate (P=0.125) did not differ significantly between the three groups before the intervention. However, there were significant differences in mean diastolic blood pressure (P<0.001) and mean pulse rate (P<0.001) in the post-intervention of the three groups.
Conclusion:
Aromatherapy treatments using rose and lavender essential oils can contribute to the stabilization of some Hemodynamic Symptoms.
Keywords: Aromatherapy, Diabetes mellitus, Hemodynamics
Copyright and License Information
© 2024 The Authors.
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
None.
Introduction
The metabolic condition known as diabetes mellitus (DM) is both serious and complex. Due to its high incidence rate, it ranks among the most significant socioeconomic concerns globally. Over the past two decades, there has been a significant increase in DM-related morbidity and mortality.1 Since 2019, estimates indicate that there are 463 million individuals worldwide living with diabetes. This number is expected to increase to 10.2% (578 million) in 2030 and 10.9% (700 million) in 2045.2 Serious complications of type 2 diabetes encompass a wide array of adverse health effects that can profoundly impact various organ systems within the body. These complications often develop over time due to poorly controlled blood sugar levels and can significantly decrease an individual’s quality of life.1,3
Diabetes can potentially disrupt the hemodynamic balance of the body, leading to cardiovascular complications. Variations in blood pressure, heart rate, and overall circulation are often referred to as hemodynamic symptoms.4 Arterial stiffness is a common hemodynamic alteration associated with diabetes. Age, heart rate, and mean arterial pressure collectively contribute to its manifestation. Studies have revealed that hypertensive individuals with diabetes exhibit higher arterial stiffness in comparison to their non-diabetic counterparts.5 The significant hemodynamic irregularities induced by acute hyperglycemia in recently diagnosed type 2 diabetic patients are not reliant on endogenous insulin, but they can be prevented by glutathione and reversed by L-arginine. These observations suggest a disturbance in the availability of endogenous nitric oxide (NO). These findings have the potential to enhance our comprehension of the adverse cardiovascular impacts associated with episodes of increased blood sugar levels.6
Two distinct categories of interventions, encompassing pharmacological and non-pharmacological treatments, are utilized to relieve the hemodynamic symptoms experienced by these patients.3 In contemporary times, there is a significant emphasis on the integration of complementary and non-pharmacological therapies into the healthcare system, owing to their dramatic increase in acceptance. These therapies have a longstanding history of being employed to decelerate the aging process, halt disease progression, uphold overall health and wellness, and address or ameliorate both physical and mental concerns. Non-pharmacological or complementary approaches frequently entail minimal risks and adverse effects, making them suitable for standalone use or in combination with other strategies.7 Aromatherapy is a complementary therapy that uses essential oils to promote physical and emotional well-being.8 Aromatherapy commonly utilizes essential oils extracted from rosemary and lavender. Rosemary-derived essential oil is made from flower and leaf extracts, resulting in a fragrant blend characterized by a mild, herbaceous, and delightful aroma. Research has revealed that inhaling rosemary essential oil enhances short-term memory and potentially harbors antibacterial and anti-inflammatory properties.9 Lavender essential oil boasts a floral, herbaceous, and subtly lemony scent, earning recognition for its remarkable ability to alleviate anxiety and promote a sense of relaxation upon inhalation. Furthermore, this oil is believed to potentially possess antibacterial and anti-inflammatory properties.10 In one study, the impact of topically applied lavender aromatherapy on the discomfort associated with insulin injections in diabetic patients was examined.11 Furthermore, a randomized clinical experiment examined the impact of aromatherapy massage using lavender essential oil on neuropathic pain and quality of life in patients with diabetes.12
Conducting research is imperative to advance scientific understanding, establish evidence-based treatment alternatives, enrich patient-centered care, explore alternative therapies, and potentially improve preventive care strategies. So, this study aimed to conduct a comparative analysis of the therapeutic impacts of rose and lavender aromatherapy on hemodynamic symptoms among individuals with a recent diabetes diagnosis.
Methods
Patients
This cross-over controlled clinical trial study was performed on diabetic patients who sought care at Hormoz Clinic in Bandar Abbas during a specified time frame of their clinic visits. Sample selection was based on a non-random convenience sampling method within the period spanning from October 2022 to November 2022. Adhering to inclusion criteria and completion of patient satisfaction forms by the patient or their accompanying individual, participants were allocated to the three groups (“rose inhalation,” “lavender inhalation,” and “control group”) using a random block approach consisting of six blocks, as depicted by the extraction codes detailed in Figure 1.
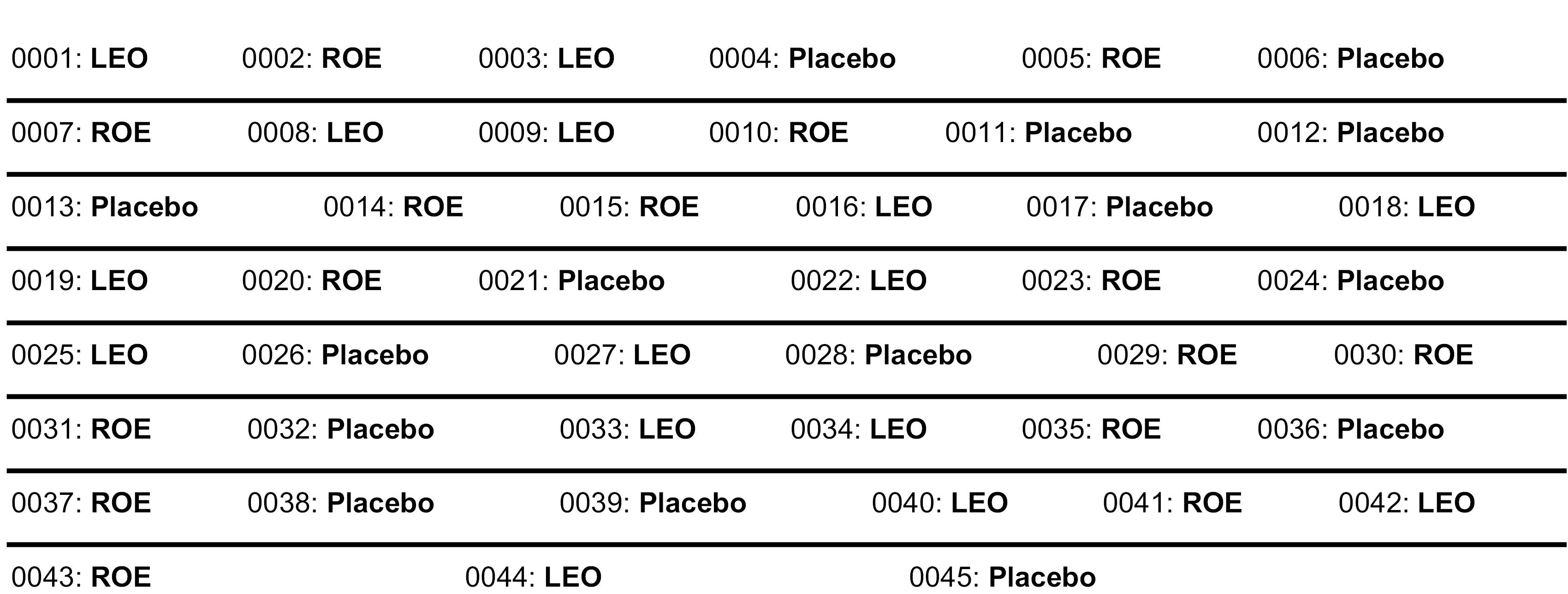
Figure 1.
Random sequence generated with 6 blocks using randomization maine software
.
Random sequence generated with 6 blocks using randomization maine software
To calculate the sample size, based on the study of Akhavan-Abiri et al,13 the sample size was determined using G*Power software version 3.1.2.9 based on the formula for calculating the sample size for two independent groups, resulting in 10 participants per group. Moreover, to calculate the sample size for three independent groups, the sample size for each group was estimated to be approximately 15 individuals for the three distinct groups, where ‘k’ represents the number of compared groups, in this case, three groups.
In this study, the inclusion criteria were having a verified medical record indicating diabetes by a physician, being diagnosed with diabetes within the past three months, being within the age range of 18 to 65 years, having the physical and mental ability to respond to questions, and being aware of time, location, and people. The exclusion criteria were sensitivity to odorous plants, a history of allergies and respiratory illness, disturbances in consciousness level, olfactory disorders, dissatisfaction after inhalation, hemodynamic instability during the intervention (including signs of anaphylactic shock, severe fluctuations in blood pressure, blood sugar, and any severe disorder requiring immediate intervention in vital signs), participant’s unwillingness to continue participation in the study, and mortality, as well as having chronic diabetes-related complications.
Initially, the researcher conducted group sessions by attending the clinic to introduce and explain the implementation process of the plan to the patients. During the orientation session, explanations regarding the execution methods, the research objectives, and the introduction of aromatherapy with lavender and rose oil were provided, aiming to establish insight and readiness for active participation in the upcoming sessions. Subsequently, they were asked to complete the sociodemographic information form made by the researcher, which included age, gender, marital status, occupation, type of diabetes, and time of diabetes diagnosis. In this study, participants were blinded to the study group they were assigned to. Before implementing the aromatherapy method, the researcher obtained sufficient information in these areas and then proceeded with the interventions. In each group, questionnaires were completed by the patients before the intervention. Two drops of 10% lavender essential oil (obtained from Barij Essence Pharmaceuticals) were placed on a 10 × 10 cm handkerchief for the lavender group and placed at a distance of 20 cm from the participants’ noses, attached to their clothing. Similarly, in the rose oil group, the same amount of 10% rose essential oil was applied to a 10 × 10 cm handkerchief and attached to the participants’ clothing at a 20-cm distance from their noses. The participants inhaled the aroma for 20 minutes.
The control group was also exposed to a placebo (an inert odorless oil) using the same method. The intervention took place in three sessions. In the first session, aromatherapy intervention with rose essential oil was performed for the first group, aromatherapy intervention with lavender essential oil was given to the second group, and the third group received the placebo. Immediately after the 20-minute intervention, the physiological indicators of the patients were measured and recorded. To avoid transferring treatment effects from the first stage to the second stage, a one-week washout period or cleansing period was implemented.
In the second session, for the group that had received aromatherapy intervention with lavender essential oil in the first session, aromatherapy intervention with rose essential oil was administered, the group that had received aromatherapy intervention with rose essential oil in the first session, a placebo (an inert odorless oil) was used in this session. Furthermore, in the group that had been in the control group in the first session, aromatherapy intervention with lavender essential oil was conducted at this stage. Immediately after the 20-minute intervention, physiological indicators were measured and recorded. To prevent the transfer of treatment effects from the second stage to the third stage, a one-week washout period was implemented. In the third session, the group that had received aromatherapy intervention with rose essential oil in the second session, this session was replaced with the placebo group. For the group that had received aromatherapy intervention with lavender essential oil in the second session, aromatherapy intervention with rose essential oil was performed in this session. For the group that had received a placebo in the second session, aromatherapy intervention with lavender essential oil was performed in this session. Additionally, it was ensured that during the interventions, the researcher or intervention provider did not use any perfumes or colognes.
Tools used for measuring physiological indices include the BOSCH + SOHN (BOSO) blood pressure monitor, manufactured in Germany (2017), with a serial number (4002427015021), which was utilized for measuring systolic and diastolic blood pressure. The JUMPER JPD-500A pulse oximeter from China (2017), with a serial number (6951740544443), was employed for measuring arterial blood oxygen saturation. The Meheconova thermometer, made in China (2016), with a serial number (20161230), was used for measuring body temperature. The Littmann Classic II stethoscope, produced in the United States (2017), with a serial number (4710636648410), was utilized for auscultating sounds related to systolic and diastolic blood pressure measurements. The Q and Q HS43 chronometer from Japan (2017), with a serial number (8809126644301), was employed for counting respiratory rate and heart rate.
Data analysis was performed using statistical software Stata version 14.0 and SPSS version 26. To examine the intervention effect, transfer effect, time effect, and a cross-sectional data analysis test (a variance-based analysis) were employed. A one-way analysis of variance (ANOVA) test was utilized to compare the mean systolic and diastolic blood pressure, as well as the pulse rate, among the three distinct recipient groups of interventions for each period. Furthermore, the post hoc Bonferroni test was applied after achieving significance in the ANOVA test, for comparison of the mean pairs of groups. In all statistical tests, a significance level of P < 0.05 was considered statistically significant.
Results
The results reveal that in the lavender group, the male percentage is approximately 53.3%, while in both the control group and the rose group, male percentages are noted at 46.7%. Moreover, the majority of individuals in the control group (86.7%), lavender group (86.7%), and rose group (80%) were married. The results of this analysis indicated that there was a significantly better reduction in diastolic blood pressure with the lavender intervention compared to rose, and in comparison, to the control group, they showed a significantly better effect (P < 0.001) (Table 1).
Table 1.
Comparison of mean diastolic blood pressure among study participants, stratified by intervention sequence in three periods
Before intervention
(After randomly assigning 45 people to three groups)
|
First period
|
Second period
|
Third period
|
Results of ANOVA with repeated measures
|
|
(Sequence)
|
Mauchly’s test (
P
value)
|
F*
|
P
value
|
Rose (n = 15)
76.73 ± 4.49 |
Rose
69.13 ± 4.96 |
Rose
71.80 ± 5.28 |
Rose
70.78 ± 5.38 |
L- > Co- > R |
< 0.001 |
10.93 |
0.001 |
Lavender (n = 15)
78.60 ± 3.99 |
Lavender
71.20 ± 4.50 |
Lavender
70.00 ± 5.55 |
Lavender
69.66 ± 4.28 |
Co- > R- > L |
< 0.001 |
14.03 |
< 0.001 |
Control (n = 15)
77.67 ± 3.63 |
Control
76.00 ± 3.68 |
Control
76.60 ± 3.90 |
Control
76.73 ± 5.28 |
R- > L- > Co |
< 0.001 |
11.01 |
< 0.001 |
F = 0.796
P = 0.459 |
F = 9.56
< 0.001 |
F = 7.08
0.002 |
F = 8.55
0.001 |
-
|
-
|
-
|
-
|
L: lavender; R: rose; C: control; *The Greenhouse-Geisser Correction.
For the three pathways or sequences, following the triple interventions, each of the three groups exhibits a decreasing trend in systolic blood pressure of diabetic patients up to the second period. However, this reduction was more pronounced, respectively, for patients categorized as controls and receiving the rose intervention, compared to those experiencing the lavender intervention. Nonetheless, statistically significant differences in the mean systolic blood pressure among these three groups during this period were not observed (P = 0.908).
Subsequently, in the second period, patients placed in the control group experienced the highest blood pressure, while the two groups of patients treated with rose and lavender interventions experienced the lowest blood pressure. In the third period as well, similar to the second period, patients undergoing rose and lavender interventions experienced a greater reduction in systolic blood pressure compared to the control group. To compare the mean changes in systolic blood pressure within the pathways (sequences), a repeated measures analysis of variance was employed. The results demonstrated that the trend of changes in systolic blood pressure within the three pathways, namely: R- > L- > Co (P = 0.104), L- > Co- > R (P = 0.067), and Co- > R- > L (P = 0.117), did not exhibit statistically significant differences (Table 2).
Table 2.
Comparison of mean systolic blood pressure among study participants, stratified by intervention sequence in three periods
Before intervention
(After randomly assigning 45 people to three groups)
|
First period
|
Second period
|
Third period
|
Results of ANOVA with repeated measures
|
|
(Sequence)
|
Mauchly’s test (
P
value)
|
F*
|
P
value
|
Rose (n = 15)
10.81 ± 127.07 |
Rose
27.06 ± 13.121 |
Rose
121.46 ± 15.22 |
Rose
121.40 ± 14.40 |
L- > Co- > R |
< 0.001 |
2.19 |
0.104 |
Lavender (n = 15)
129.13 ± 12.72 |
Lavender
123.73 ± 16.73 |
Lavender
109.00 ± 16.74 |
Lavender
123.73 ± 16.92 |
Co- > R- > L |
< 0.001 |
2.57 |
0.067 |
Control (n = 15)
128.13 ± 14.73 |
Control
109.00 ± 30.64 |
Control
123.73 ± 16.73 |
Control
126.60 ± 10.30 |
R- > L- > Co |
< 0.001 |
2.08 |
0.117 |
0.097 = F
P = 0.908 |
F = 1.98
P = 0.15 |
F = 1.43
P = 0.250 |
F = 0.514
P = 0.602 |
- |
- |
- |
- |
L: lavender; R: rose; C: control; *The Greenhouse-Geisser Correction.
The statistical results showed no significant difference in the number of pulses among the three groups, and the means were homogeneous (P = 0.125) at the beginning of the study. After the intervention in the first period, changes in the number of pulses for the rose and lavender groups were statistically significant, with the mean pulse decreasing in these two groups and increasing in the control group (P = 0.951). In the second period, the number of pulses for the rose group was significantly lower than the lavender group (P = 0.019). In this period, the rose group did not show any significant change compared to the lavender and control groups. In the third period, the number of pulses for the lavender group was significantly lower than both the rose and control groups (P = 0.024). Additionally, mean comparisons indicated that the rose group had a significantly lower number of pulses than the control group (P= 0.020), and the lavender group had a significantly lower number of pulses than the control group (P = 0.624). The trend of changes in the number of pulses within the pathways (sequences) was analyzed using repeated measures analysis of variance. The results demonstrated that when both rose and lavender interventions were employed, a decreasing trend in the number of pulses of patients was observed within all three pathways, and this reduction was statistically significant for all three pathways (P < 0.001) (Table 3).
Table 3.
Comparison of mean heart rate among study participants, stratified by intervention sequence in three periods
|
Before intervention (After randomly assigning 45 people to three groups)
|
First period
|
Second period
|
Third period
|
Results of ANOVA with repeated measures
|
|
Sequence
|
Mauchly’s test (
P
value)
|
F*
|
P
value
|
Rose (n = 15)
92.40 ± 16.63 |
Rose
81.86 ± 19.70 |
Rose
72.00 ± 19.92 |
Rose
83.07 ± 20.67 |
L- > Co- > R |
0.029 |
44.78 |
< 0.001 |
Lavender (n = 15)
93.80 ± 19.70 |
Lavender
81.60 ± 21.22 |
Lavender
82.73 ± 15.87 |
Lavender
71.53 ± 21.49 |
Co- > R- > L |
0.001 |
27.94 |
< 0.001 |
Control (n = 15)
81.26 ± 17.27 |
Control
81.66 ± 17.50 |
Control
91.93 ± 19.46 |
Control
92.40 ± 17.58 |
R- > L- > Co |
0.272 |
55.71 |
< 0.001 |
F = 2.18
P = 0.125 |
F = 2.05
P = 0.951 |
F = 4.36
P = 0.019 |
F = 4.10
P = 0.024 |
- |
- |
- |
- |
L: lavender; R: rose; C: control. *The Greenhouse-Geisser Correction
Discussion
The primary objective of this study was to determine and compare the effects of rose and lavender aromatherapy on the hemodynamic symptoms of diabetic patients with recent diagnoses of diabetes. The results of the present study indicated that the mean diastolic blood pressure did not significantly differ between the control group and the rose and lavender aromatherapy groups before the implementation of interventions. However, during the first, second, and third phases of the study, the mean diastolic blood pressure showed significant differences among the three groups. In such a way that the mean diastolic blood pressure in the intervention groups was lower than the control group during the first, second, and third phases of the study. Moreover, the performance of the lavender aroma in reducing diastolic blood pressure was superior to the rose aroma. This reduction was statistically significant during the second phase of the study but was not significant during the first and third phases. Additionally, the sequence in which patients initially received control, followed by rose in the second phase, and lavender in the third phase, demonstrated better performance of aromatherapy interventions in reducing diastolic blood pressure.
The findings of the current study are consistent with previous studies investigating the effect of rose scent on diastolic blood pressure in various patient populations, including the study by Madadkar Dehkordi,14 Shirzad et al,15 and Mohamadinasab et al,16 which all reported a reduction in diastolic blood pressure after aromatherapy with rose aroma. However, these results contradict the study by Franco et al.17 This contradiction may be attributed to differences in study methodology and sample populations between the two studies. The present study is considered to have a superior methodological design compared to the mentioned study. Nevertheless, systematic review studies and meta-analyses are necessary to address this inconsistency.
The results of the present study showed no significant differences in systolic blood pressure among the control group, rose aromatherapy group, and lavender aromatherapy group before implementing the interventions and during the first, second, and third phases of the study. Although the reduction in systolic blood pressure was greater in the rose and lavender aromatherapy groups compared to the control group, this reduction was not statistically significant. These findings are inconsistent with previous studies investigating the effect of rose scent on systolic blood pressure in various patient populations, including the studies by Madadkar Dehkordi,14 Shirzad et al,15 and Mohamadinasab et al,16 which demonstrated a significant reduction in systolic blood pressure following rose aromatherapy.
However, the results of this study are not consistent with the study by Moradi et al18 and Teymouri et al.19 Since the present study is the first of its kind to compare the effects of rose and lavender scents on blood pressure in diabetic patients, it carries novelty in this regard. However, further studies with larger sample sizes are highly necessary to resolve such discrepancies. Additionally, one possible reason for these inconsistencies may be the small sample size of the present study.
The results of the present study showed no significant differences in the average number of pulses among the control group, rose aromatherapy group, and lavender aromatherapy group before implementing the interventions. However, during the second and third phases of the study, there were significant differences in the average number of pulses among the three groups. Specifically, the average number of pulses in the intervention groups was lower than the control group during the second and third phases of the study. This reduction was significantly greater in the rose aromatherapy group during the second phase and in the lavender aromatherapy group during the third phase. The trend of pulse changes within the groups followed a decreasing pattern, indicating that when both rose and lavender interventions were applied, a decreasing trend in the number of pulses was observed in all three groups, and this reduction was statistically significant in all three groups. The result suggests that although the performance of rose and lavender in reducing the number of pulses in patients was relatively similar, it is preferable compared to a non-intervention state.
The findings of the present study are consistent with previous studies examining the effects of rose aroma on the average number of pulses in different patient populations, including the study by Madadkar Dehkordi14 and the study by Shirzad et al,15 which reported a reduction in the average number of pulses following rose aromatherapy. Additionally, the present findings align with the results of previous studies investigating the impact of lavender aroma on the average number of pulses in various patient populations, such as the study by Moradi et al,18 which demonstrated a reduction in the average number of pulses after lavender aromatherapy. These consistent findings indicate the positive influence of rose and lavender aromatherapy, similar to nursing interventions, on the number of pulses, which is an essential variable in assessing the hemodynamic status of patients. In this regard, considering the easily measurable nature of pulse rate as a representative of physiological indices and the impact of alleviative interventions on it, it can be concluded that the pulse rate changes before the endoscopic procedure. Therefore, it is suggested as a clinical indicator. However, for further comparison, the design and implementation of clinical trials examining the effects of aroma therapy on physiological indices in different populations is strongly recommended.
Study Highlights
What is current knowledge?
What is new here?
-
The novelty lies in the direct comparison of rose and lavender aromatherapy, the sequential intervention design, the focus on newly diagnosed diabetic patients, and the phase-specific and comprehensive assessment of hemodynamic parameters.
Conclusion
Both the systolic and diastolic blood pressure, as well as the pulse rate, decreased in both the rose and lavender aromatherapy groups following the intervention, indicating the positive effect of both methods in reducing physiological indices. Therefore, both rose and lavender aromatherapy can be utilized as complementary modalities for improving physiological indicators in this specific population.
Competing Interests
The authors declare that they have no competing interests.
Ethical Approval
The procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all the patients or their parents/legal guardians. This research project was approved by the Research Ethics Committees of Hormozgan University of Medical Sciences (Ethics No. IR.HUMS.REC.1401.292). This study is registered in Iranian Registry of Clinical Trials (identifier: IRCT20230104057049N1).
References
- Tomic D, Shaw JE, Magliano DJ. The burden and risks of emerging complications of diabetes mellitus. Nat Rev Endocrinol 2022; 18(9):525-39. doi: 10.1038/s41574-022-00690-7 [Crossref] [ Google Scholar]
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019; 157:107843. doi: 10.1016/j.diabres.2019.107843 [Crossref] [ Google Scholar]
- Suryasa IW, Rodríguez-Gámez M, Koldoris T. Health and treatment of diabetes mellitus. Int J Health Sci 2021; 5(1):1-5. doi: 10.53730/ijhs.v5n1.2864 [Crossref] [ Google Scholar]
- International Hypoglycaemia Study Group. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management. Lancet Diabetes Endocrinol 2019; 7(5):385-96. doi: 10.1016/s2213-8587(18)30315-2 [Crossref] [ Google Scholar]
- Agnoletti D, Lieber A, Zhang Y, Protogerou AD, Borghi C, Blacher J. Central hemodynamic modifications in diabetes mellitus. Atherosclerosis 2013; 230(2):315-21. doi: 10.1016/j.atherosclerosis.2013.07.054 [Crossref] [ Google Scholar]
- Jamalnia S, Javanmardifard S, Akbari H, Sadeghi E, Bijani M. Association between cognitive impairment and blood pressure among patients with type II diabetes mellitus in southern Iran. Diabetes Metab Syndr Obes 2020; 13:289-96. doi: 10.2147/dmso.s238247 [Crossref] [ Google Scholar]
- Wang X, Kang J, Liu Q, Tong T, Quan H. Fighting diabetes mellitus: pharmacological and non-pharmacological approaches. Curr Pharm Des 2020; 26(39):4992-5001. doi: 10.2174/1381612826666200728144200 [Crossref] [ Google Scholar]
- Farrar AJ, Farrar FC. Clinical aromatherapy. Nurs Clin North Am 2020; 55(4):489-504. doi: 10.1016/j.cnur.2020.06.015 [Crossref] [ Google Scholar]
- Sulung N, Aulia FF. Effect of rosemary aromatherapy (Rosmarinus officinalis) to memory of short-term memory in elderly. Jurnal Endurance 2018; 3(2):247-52. doi: 10.22216/jen.v3i2.1216 [Crossref] [ Google Scholar]
- Jafari-Koulaee A, Elyasi F, Taraghi Z, Ilali ES, Moosazadeh M. A systematic review of the effects of aromatherapy with lavender essential oil on depression. Cent Asian J Glob Health 2020; 9(1):e442. doi: 10.5195/cajgh.2020.442 [Crossref] [ Google Scholar]
- Demirağ H, Hintistan S, Bulut E. The effect of topically administered lavender aromatherapy on the pain of insulin injection in diabetic patients: a double-blind randomized controlled clinical trial. Turk J Med Sci 2022; 52(6):1845-53. doi: 10.55730/1300-0144.5531 [Crossref] [ Google Scholar]
- Rivaz M, Rahpeima M, Khademian Z, Dabbaghmanesh MH. The effects of aromatherapy massage with lavender essential oil on neuropathic pain and quality of life in diabetic patients: a randomized clinical trial. Complement Ther Clin Pract 2021; 44:101430. doi: 10.1016/j.ctcp.2021.101430 [Crossref] [ Google Scholar]
- Akhavan-Abiri F, Shairi MR, Gholami Fesharaki M. The relationship between attachment and psychological distress with regard to the mediating role of mindfulness. Feyz 2019;23(1):89-101. [Persian].
- Madadkar Dehkordi S. Effect of aromatherapy with rosemary essential oil on preoperative anxiety, stress, depression and physiological parameters in candidates for general surgery: a clinical trial. Complementary Medicine Journal 2022; 12(2):148-59. doi: 10.32598/cmja.12.2.671.4 [Crossref] [ Google Scholar]
- Shirzad M, Nasiri E, Hesamirostami MH, Akbari H. Comparing the effects of rose essential oil and Benson relaxation technique on preoperative anxiety and hemodynamic status and postoperative complications in rhinoplasty candidates. Complementary Medicine Journal 2021; 11(2):180-91. doi: 10.32598/cmja.11.2.1077.1 [Crossref] [ Google Scholar]
- Mohamadinasab S, Ravari A, Mirzaei T, Sayadi A. The effect of aromatherapy with essential rose oils on blood pressure in hypertensive patients. J Med Plants 2019; 18(72):202-14. doi: 10.29252/jmp.4.72.202.[Persian] [Crossref] [ Google Scholar]
- Franco L, Blanck TJ, Dugan K, Kline R, Shanmugam G, Galotti A. Both lavender fleur oil and unscented oil aromatherapy reduce preoperative anxiety in breast surgery patients: a randomized trial. J Clin Anesth 2016; 33:243-9. doi: 10.1016/j.jclinane.2016.02.032 [Crossref] [ Google Scholar]
- Moradi K, Ashtarian H, Darabi F, Hashemian AH, Saifi F. A survey on the effects of Lavender aromatherapy on the anxiety and vital signs of patients with ischemic heart diseases hospitalized in cardiac intensive care units. J Clin Res Paramed Sci 2016; 4(4):e82067. [ Google Scholar]
- Teymouri F, Rajai N, Farsi Z, Pourmirzai M. The effects of inhaling lavender fragrance on stress and anxiety during sheath take out in patients after coronary angiography. J Med Plants 2019; 18(72):78-89. doi: 10.29252/jmp.4.72.S12.78.[Persian] [Crossref] [ Google Scholar]