J Res Clin Med. 12:27.
doi: 10.34172/jrcm.34552
Original Article
Risk factors of type II diabetes among bankers of Kathmandu Metropolitan city: A cross-sectional study
Sailendra Thapa Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, * 
Prakriti Koirala Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – review & editing, 2
Author information:
1Department of Public Health, Nepalese Army Institute of Health Sciences, Tribhuvan University, Nepal
2Patan Academy of Health Sciences, Nepal
Abstract
Introduction:
Identifying the risk factors of type 2 diabetes (T2DM) among the most vulnerable people is crucial as it helps to prevent complications and improve health outcomes. The job of bank employees is both sedentary and accompanies high levels of mental stress, making them more susceptible to non-communicable disease like diabetes. This study aims to identify the prevalence of risk factors of T2DM among bank employees.
Methods:
A cross-sectional study was conducted among 348 bank employees from selected banks of Kathmandu Metropolitan City, the largest and capital city of Nepal from October to December 2020. Pre-tested, self-administered structured questionnaire based on the WHO STEP Instrument and Perceived Stress Scale was used for the data collection. Data was analyzed using SPSS version 22.0 software.
Results:
The mean age of respondents was 34.8±8.9 years. At least, one risk factor was present among all the respondents, whereas 22.4% having had over four risk factors. The most common risk factor was improper dietary habits (99.4%). Similarly, 84.2% of the respondents had moderate to high levels of perceived stress. Factors like age, gender, level of education, marital status, socio-economic status, and family history were associated with the risk factors of T2DM.
Conclusion:
The findings of this study revealed that bankers were at high risk of T2DM. This study showed an urgent need to bring the attention of the concerned authorities to promote a healthy lifestyle, create a stress-free work environment, and awareness about the risk of T2DM among bankers, coming up with public health strategies for its prevention.
Keywords: Diabetes mellitus, Nepal, Risk factors, Sedentary behavior
Copyright and License Information
© 2024 The Authors.
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This study has not been supported financially by any person or organization.
Introduction
Diabetes mellitus, a chronic metabolic condition, and a major public health issue, is the leading cause of mortality and morbidity worldwide.1,2 Global estimates show the 9.3% prevalence of diabetes in 2019 (463 million) which will be raised to 10.2% (578 million) and 10.9% (700 million) by 2030 and 2045, respectively.3 Moreover, a systematic review states 8.5% prevalence of diabetes in Nepal.4 Diabetes is characterized by elevated blood glucose levels resulting from either lacking of the insulin production or insulin resistance.5 The most common form of diabetes is type 2 diabetes (T2DM).
Because of rapid mechanization in the agricultural and industrial sectors, most of the physical works have been shifted to less effort-required work. According to the Sedentary Behavior Research Network, the proportion of physical inactivity is increasing among the working population because of their job entity of table work.6 Several studies have shown an association between sedentary lifestyle and the development of obesity, cardiovascular diseases, and T2DM.7-9 In this regard, the working nature of bank employees is both sedentary and involves high levels of stress,10 increasing the chance of T2DM, and subsequently decreasing the quality of life.11 This group of people spend almost all their working hours sitting in the same place with a high-level of mental stress. The study conducted among bankers of Zambia showed a 15% prevalence of T2DM higher than the government employees in India.10 Different studies also conducted among bankers and similar sectors of physically less demanding office jobs found overweight, age (45 and older), lack of physical activity, having a family member with T2DM, and stress as major prevalent risk factors for T2DM.10,12-14 However most of the studies indicating the risk factor of T2DM among bankers have been conducted in developed countries. In this regard, the primary objective of this study is to identify risk factors of T2DM among bank employees of selected banks in Kathmandu metropolitan city, Nepal, one of the least developed countries. Having knowledge of T2DM risk factors among bank employees helps with primary prevention, improving health outcomes and quality of life, as well as reducing the economic burden. Early identification of risk factors helps to increase healthcare-seeking behavior15 among the employees, which in turn, increases the efficiency within the working station.
Methods
A cross-sectional study was conducted among 348 bank employees from selected banks of Kathmandu Metropolitan City, Nepal. Out of a total of 27 class ‘A’ commercial banks, 3 banks were selected randomly. The number of respondents from each bank was determined using a population proportionate sampling technique and each respondent was selected using a systematic sampling method. All the administrative employees of age group 20-69 were included in the study while pregnant women were excluded from this study.
The research proposal was approved by the Institutional Review Committee (IRC) of the Manmohan Memorial Institute of Health Sciences, Nepal. Written informed consent was taken from each participant and permission for data collection was also taken from each bank. The data was collected from October to December 2020 using a self-administered structured questionnaire which was based on the WHO STEP Instrument16 and Perceived Stress Scale.17 Pre-testing of the questionnaire was performed at SBI Bank of Lalitpur Metropolitan City. Also, the questionnaire was prepared in English and translated into Nepali and back-translated to English to ensure linguistic validity by different researchers. Six known risk factors of T2DM (smoking, alcohol consumption, physical activity, dietary habit, family history of diabetes, and stress) along with the socio-demographic characteristics of the respondents were assessed in the study. This study was conducted during a semi-lockdown situation due to the COVID-19 pandemic. In hence, to maintain social distancing and to decrease the risk of COVID-19, BMI could not be assessed, although many studies found it as one of the major risk factors of T2DM. Data was entered, analyzed, and interpreted according to the objective of the study using SPSS version 22.0 software. The results obtained were expressed as mean, frequency, and percentages. Cross tabulation, chi-square test, and binary logistic regression analysis were also utilized to determine the association at 95% level of confidence.
Results
The socio-demographic characteristics of the respondents are shown in Table 1. The mean age of respondents was 34.8 ± 8.951. Out of 348 individuals, 55% were male and 46.8% of the respondents had a post-graduate degree. In addition, 64.1% of them were married and the majority belonged to the Brahmin/Chhetri community (66.7%). 55.7% lived in the nuclear family and almost all of the respondents were above the poverty line (94.5%).
Table 1.
Socio-demographic characteristics
|
Variables
|
Frequency
|
Percent
|
| Age group |
|
|
| Mean ± SD |
34.8 ± 8.951 |
|
| ≤ 40 |
261 |
75 |
| > 40 |
87 |
25 |
| Gender |
|
|
| Male |
192 |
55.2 |
| Female |
156 |
44.8 |
| Level of education |
|
|
| High school |
40 |
11.5 |
| Undergraduate |
145 |
41.7 |
| Post-graduate |
163 |
46.8 |
| Marital status |
|
|
| Unmarried |
104 |
29.9 |
| Married |
223 |
64.1 |
| Divorced |
21 |
6.0 |
| Ethnicity |
|
|
| Brahmin/Chhetri |
232 |
66.7 |
| Janajati |
103 |
29.6 |
| Others |
13 |
3.7 |
| Type of family |
|
|
| Nuclear |
194 |
55.7 |
| Joint |
154 |
44.3 |
| Socio-economic status |
|
|
| Above poverty line |
329 |
94.5 |
| Below poverty line |
19 |
5.5 |
The behavioral characteristics of the respondentshave been shown inTable 2. About 11.8% of all respondents were tobacco users in the form of smoking with the average age of 22.95 years old. Among the total of 348 respondents, 99.4% ate less than five portions of fruit and vegetables a day with 19% of the respondents adding salt to their food.
Table 2.
Behavioral characteristics of the respondents
|
Factors
|
Frequency
|
Percent
|
| Tobacco use (in the form of smoking) |
|
|
| Current tobacco users |
41 |
11.8 |
| Never Consumed tobacco |
307 |
88.2 |
| Current daily tobacco users (n = 41) |
41 |
100 |
| Alcohol consumption |
|
|
| Current alcohol consumption |
84 |
24.1 |
| Never consumed alcohol |
264 |
75.9 |
| Diet |
|
|
| Who ate less than 5 servings of fruit and vegetable on average per day |
346 |
99.4 |
| Who always or often add salt to the food |
66 |
19.0 |
| Who always or often eat processed food high in salt |
69 |
19.8 |
| Physical Activity |
|
|
| Engaging in physical activity |
268 |
77.1 |
| Not engaging in physical activity |
80 |
22.9 |
| Family history |
|
|
| Risk due to family history of diabetes |
80 |
23.0 |
| Father with diabetes |
24 |
30 |
| Mother with diabetes |
44 |
55 |
| Both parents with diabetes |
12 |
15 |
| Perceived stress |
|
|
| Low stress |
55 |
15.8 |
| Moderate stress |
263 |
75.6 |
| High stress |
30 |
8.6 |
The association between the demographic variables and the behavioral risk factors is shown in Table 3. Age was found to be associated with tobacco consumption (P < 0.001) and alcohol consumption (P < 0.001). There was no association between tobacco consumption and marital status (P = 0.162), ethnicity (P = 0.628), type of family (P = 0.06), and socio-economic status (P = 0.365). Similarly, a significant association was also found between consumption of alcohol and other socio-demographic variables such as gender (P < 0.001), level of education (P = 0.008), and marital status (P = 0.022). Also, there was no significant association between alcohol consumption and ethnicity, type of family, and socio-economic status. Of note, family history (P = 0.042) was found to be associated with socio-economic status, too. No association was observed between stress and socio-demographic variables (P > 0.05).
Table 3.
Association between socio-demographic and behavioral characteristics of the respondents
|
Factors
|
Tobacco
|
Alcohol
|
Physical activity
|
Family history
|
Stress
|
Y
n (%)
|
N
n (%)
|
P
value
|
Y
n (%)
|
N
n (%)
|
P
value
|
Y
n (%)
|
N
n (%)
|
P
value
|
Y
n (%)
|
N
n (%)
|
P
value
|
Y
n (%)
|
N
n (%)
|
P
value
|
| Age |
|
|
< 0.001 |
|
|
< 0.001 |
|
|
1.0 |
|
|
0.556 |
|
|
0.149 |
| ≤ 40 |
20 (7.7) |
241 (92.3) |
|
49 (18.8) |
212 (81.2) |
|
201 (77.0) |
60 (23.0) |
|
62 (23.8) |
199 (76.2) |
|
224 (85.8) |
37 (14.2) |
|
| > 40 |
21 (24.1) |
66 (75.9) |
|
35 (40.2) |
52 (59.8) |
|
67 (77.0) |
20 (23.0) |
|
18 (20.7) |
69 (79.3) |
|
69 (79.3) |
18 (20.7) |
|
| Gender |
|
|
N/A |
|
|
< 0.001 |
|
|
0.421 |
|
|
0.633 |
|
|
0.280 |
| Male |
41 (21.4) |
151 (78.6) |
|
73 (38.0) |
119 (62.0) |
|
151 (78.6) |
41 (21.4) |
|
46 (24.0) |
146 (76.0) |
|
158 (82.3) |
34 (17.7) |
|
| Female |
0 (0) |
156 (100) |
|
11 (7.1) |
145 (92.9) |
|
117 (75.0) |
39 (25.0) |
|
34 (21.8) |
122 (78.2) |
|
135 (86.5) |
21 (13.5) |
|
| Level of education |
|
|
0.023 |
|
|
0.008 |
|
|
0.068 |
|
|
0.655 |
|
|
0.117 |
| High school |
6 (15.0) |
34 (85.0) |
|
16 (40.0) |
24 (60.0) |
|
25 (62.5) |
15 (37.5) |
|
8 (20.0) |
32 (80.0) |
|
30 (75.0) |
10 (25.0) |
|
| College/University |
24 (16.6) |
121 (83.4) |
|
39 (26.9) |
106 (73.1) |
|
114 (78.6) |
31 (21.4) |
|
31 (21.4) |
114 (78.6) |
|
120 (82.8) |
25 (17.2) |
|
| Post-graduate |
11 (6.7) |
152 (93.3) |
|
29 (17.8) |
134 (82.2) |
|
129 (79.1) |
34 (20.9) |
|
41 (25.2) |
122 (74.8) |
|
143 (87.7) |
20 (12.3) |
|
| Marital Status |
|
|
0.162 |
|
|
0.022 |
|
|
0.482 |
|
|
0.502 |
|
|
0.289 |
| Unmarried |
7 (6.7) |
97 (93.3) |
|
15 (14.4) |
89 (85.6) |
|
77 (74.0) |
27 (26.0) |
|
28 (26.9) |
76 (73.1) |
|
83 (79.8) |
21 (20.2) |
|
| Married |
31 (13.9) |
192 (86.1) |
|
63 (28.3) |
160 (71.7) |
|
173 (85.7) |
50 (14.3) |
|
47 (21.1) |
176 (78.9) |
|
191 (85.7) |
32 (14.3) |
|
| Divorced |
3 (14.3) |
18 (85.7) |
|
6 (28.6) |
15 (71.4) |
|
18 (77.6) |
3 (22.4) |
|
5 (23.8) |
16 (76.2) |
|
19 (90.5) |
2 (9.5) |
|
| Ethnicity |
|
|
0.628 |
|
|
0.736 |
|
|
0.933 |
|
|
0.559 |
|
|
N/A |
| Brahmin/Chhetri |
30 (12.9) |
202 (87.1) |
|
56 (24.1) |
176 (75.9) |
|
180 (77.6) |
52 (22.4) |
|
51 (22.0) |
181 (78.0) |
|
194 (83.6) |
38 (16.4) |
|
| Janajati |
10 (9.7) |
93 (90.3) |
|
26 (25.2) |
77 (74.8) |
|
78 (75.7) |
25 (24.3) |
|
27 (26.2) |
76 (73.8) |
|
86 (83.5) |
17 (16.5) |
|
| Others |
1 (7.7) |
12 (92.3) |
|
2 (15.4) |
11 (84.6) |
|
10 (76.9) |
3 (23.1) |
|
2 (15.4) |
11 (84.6) |
|
13 (100.0) |
0 (0) |
|
| Type of family |
|
|
0.06 |
|
|
0.334 |
|
|
0.091 |
|
|
0.918 |
|
|
0.623 |
| Nuclear |
31 (16.0) |
163 (84.0) |
|
43 (22.2) |
151 (77.8) |
|
156 (80.4) |
38 (19.6) |
|
45 (23.2) |
149 (76.8) |
|
165 (85.1) |
29 (14.9) |
|
| Joint and extended |
10 (6.5) |
144 (93.5) |
|
41 (26.6) |
113 (73.4) |
|
112 (72.7) |
42 (27.3) |
|
35 (22.7) |
119 (77.3) |
|
128 (83.1) |
26 (16.9) |
|
| Socio-economic status |
|
|
0.365 |
|
|
0.747 |
|
|
< 0.001 |
|
|
0.042 |
|
|
0.519 |
| Above poverty line |
40 (12.2) |
289 (87.8) |
|
80 (24.3) |
249 (75.7) |
|
263 (79.9) |
66 (20.1) |
|
72 (21.9) |
257 (78.1) |
|
278 (84.5) |
51 (15.5) |
|
| Below poverty line |
1 (5.3) |
18 (94.7) |
|
4 (21.1) |
15 (78.9) |
|
5 (26.3) |
14 (73.7) |
|
8 (42.1) |
11 (57.9) |
|
15 (78.9) |
4 (21.1) |
|
Also, Table 4 indicates the binary logistic analysis of socio-demographic with behavioral factors. All the variables with P value < 0.2 were considered for the binary logistic regression analysis. The table shows that ages more than 40 years (OR = 3.834, 95% CI = 1.962-7.494) was highly associated with smoking whereas people living in the joint and extended family (OR = 0.365, 95% CI = 0.173-0.771) was found to be less likely to involved in smoking. The study shows people above the age of 40 years (OR = 2.912, 95% CI = 1.715-4.944), being male (OR = 8.086, 95% CI = 4.102-15.941), post-graduate degree (OR = 3.080, 95% CI = 1.456-6.516), and being married (OR = 2.33, 95% CI = 1.257-4.342), increase the chance of alcohol consumption. Bank employees with a college degree (OR = 2.206, 95% CI = 1.039-4.686) and post-graduate degrees (OR = 2.276, 95% CI = 1.083-4.787) had a higher chance of involving in physical activity in comparison to those with only high school education Results of additional analyses are available at supplementary file.
Table 4.
Binary logistic analysis of associated socio-demographic with behavioral risk factors
|
Factors
|
Tobacco (Smoking)
|
Alcohol
|
Physical activity
|
Family history
|
Stress
|
|
P
value
|
OR
|
95% CI
|
P
value
|
OR
|
95% CI
|
P
value
|
OR
|
95% CI
|
P
value
|
OR
|
95% CI
|
P
value
|
OR
|
95% CI
|
| Age |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| ≤ 40 |
|
Ref |
|
|
Ref |
|
|
|
|
|
|
|
|
Ref |
|
| > 40 |
< 0.001 |
3.834 |
1.962-7.494 |
< 0.001 |
2.912 |
1.715-4.944 |
- |
- |
- |
- |
- |
- |
0.152 |
0.633 |
0.339-1.182 |
| Gender |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Male |
|
|
|
|
Ref |
|
|
|
|
|
|
|
|
|
|
| Female |
- |
- |
- |
< 0.001 |
0.124 |
0.063-0.244 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
| Level of education |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| High school |
|
Ref |
|
|
Ref |
|
|
Ref |
|
|
|
|
|
Ref |
|
| Under graduate |
0.814 |
1.124 |
0.425-2.971 |
0.111 |
0.552 |
0.266-1.147 |
0.039 |
2.206 |
1.039-4.686 |
|
|
|
0.270 |
1.600 |
0.694-3.689 |
| Post graduate |
0.100 |
0.410 |
0.142-1,186 |
0.003 |
0.325 |
0.153-0.687 |
0.030 |
2.276 |
1.083-4.787 |
- |
- |
- |
0.047 |
2.383 |
1.014-5.604 |
| Marital status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Unmarried |
|
Ref |
|
|
Ref |
|
|
|
|
|
|
|
|
|
|
| Married |
0.065 |
2.237 |
0.546-9.777 |
0.007 |
2.33 |
1.257-4.342 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
| Divorced |
0.256 |
2.310 |
0.951-5.265 |
0.121 |
2.37 |
0.795-7.083 |
|
|
|
|
|
|
|
|
|
| Type of family |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Nuclear |
|
Ref |
|
|
|
|
|
Ref |
|
|
|
|
|
|
|
| Joint and extended |
0.008 |
0.365 |
0.173-0.771 |
- |
- |
- |
0.092 |
0.650 |
0.393-1.073 |
- |
- |
- |
- |
- |
- |
| Socio-economic status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Above poverty line |
|
|
|
|
|
|
|
Ref |
|
|
Ref |
|
|
|
|
| Below poverty line |
- |
- |
- |
- |
- |
- |
< 0.001 |
0.090 |
0.031-0.258 |
0.048 |
2.579 |
1.007-6.695 |
- |
- |
- |
Figure 1 represents the prevalence of risk factors of T2DM among bankers of Kathmandu Metropolitan City. Almost all the participants were having at least one risk factor for T2DM. Among the total of 348 respondents, 37.4% of them were having four risk factors whereas only 2% had one risk factor.
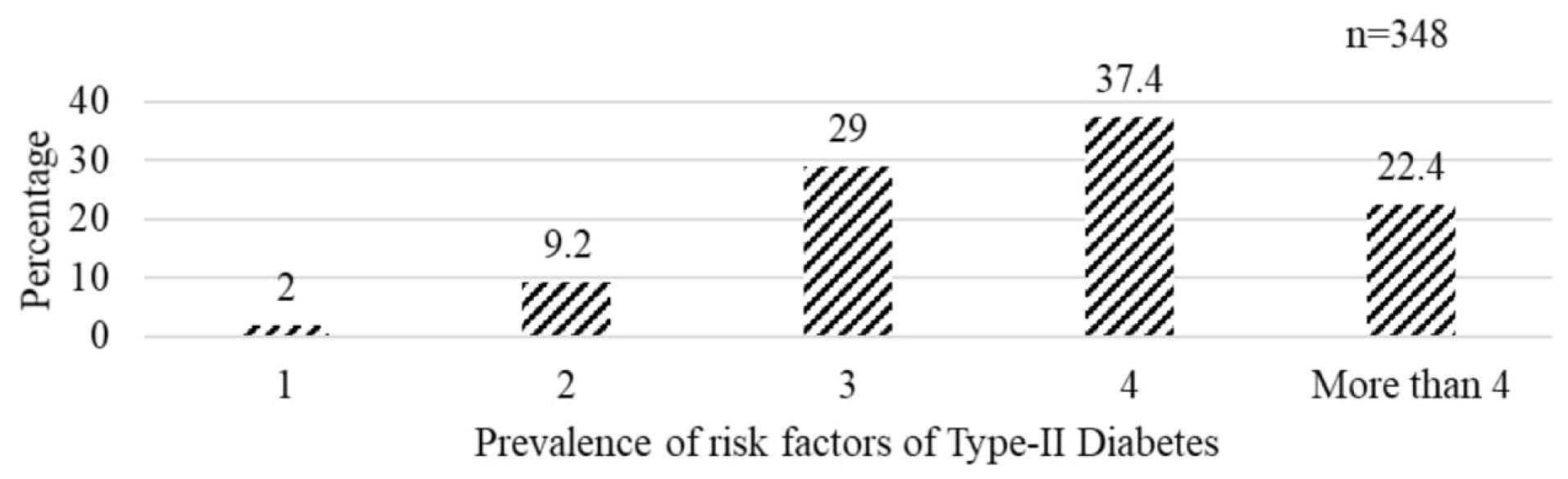
Figure 1.
Prevalence of risk factors of Type-II Diabetes
.
Prevalence of risk factors of Type-II Diabetes
Discussion
To the best of our knowledge, this is the first study conducted in Nepal to assess the prevalence of risk factors among bank employees. In this study, all of the respondents had at least one risk factor of T2DM. The most common risk factor present was the improper dietary habits like less fruit, and more processed food intake. According to the 2019 STEP Survey of Nepal, 96.7% of Nepalese individuals did not meet the WHO standard, for fruit and vegetable consumption.16 This might be due to inappropriate food culture among the Nepalese people in addition to the lack of availability and accessibility of fruits and vegetables. As this study was conducted during the semi-lockdown condition, the availability and accessibility might have been affected more.
This study revealed 11.8% prevalence of smoking among bank employees, which is similar to the result of the study conducted in India,18 but the national rate of prevalence (17.1%) is higher than this study.16 Results showed a significant association between smoking and increasing age (more than 40 years). Similar result was also demonstrated by the study conducted among bank employees of Zambia,10 India,12 and other global data.19,20 It might be because of the increasing dependency on smoking among people who have initiated it at an early age. Sometimes people might take smoking as a coping strategy for stress, which generally enhances with increasing age. An association between educational level and marital status with smoking was not found. This study found significant association between family type (joint and extended family) and smoking. Those employees who were residing in joint and extended family were less likely to be involved in smoking, which is a well-established risk factor for T2DM,21 although a study conducted in Nepal could not find an association between family type and risk of T2DM.22 This indicates that who reside in nuclear families are more vulnerable to smoking. This might be due to the limited number of family members who could give enough time to each other, therefore, people might take smoking as a socializing agent among friends.
The current study found that 24.1% of bank employees were consuming alcohol. Increasingly age (more than 40 years) was significantly associated with alcohol consumption. Alcohol is easily available and acceptable for increasing age people in comparison to young age people. Increasing age accompanied with alcohol consumption increases the chance of developing T2DM,12 while another study unlike could not establish the association between alcohol consumption and T2DM.10 Consumption of alcohol was highly associated with females. However, the result showed an inverse relation. Being female decreases the chance of consuming alcohol and increases among males, which increases the chance of developing T2DM. Although the result of this study is supported by other studies,10,23 one study showed the relationship of being female with increased alcohol consumption and risk of T2DM.24,25 Being male and consuming alcohol has been accepted as normal in Nepalese society, which might influence males to consume alcohol. A similar result was also found in the case of educational level. Increasing educational status (undergraduate and post-graduate) reduces the chance of involving in the consumption of alcohol. This might be as educational level increases, people become more aware about the harmful effects of alcohol as it increases access to information. The relation between educational status and alcohol consumption26 is well-established, increasing the risk of T2DM.22 In comparison to unmarried, married employees had a double chance of involving in alcohol consumption. The relation between marital status and the risk of T2DM is also well-explained by many studies,20,27 but unlike, the results of a study conducted in Australia revealed an association between unmarried and alcohol consumption.28 It can be explained that married people are mostly involved in social functions, rituals, and family functions, where they might get involved in alcohol consumption.
This study found that those employees with higher educational status had a higher chance of involving in physical activity. Higher educational levels might have influenced the level of awareness regarding the importance of physical activity. Therefore, a higher level of physical activity, can reduce the risk of T2DM development.10 It has also shown an increasing risk among bank employees with higher education levels.29 An association between lower socio-economic status and physical activity was also found by this study. Those with lower economic status were less likely to be involved in physical activity than those with higher economic status. Physically less active people are at the risk of developing T2DM. A study conducted in India supports this result.12 Family history of diabetes was also found to be significantly associated with lower socio-economic status. In addition, 15% of the employees having had a history of diabetes in both parents. This finding is in line with another study conducted among bank employees.12
Similarly, an association between post-graduate education and stress status was also found. With an increasing educational level, the stress level also increases among the employees of the bank, which is directly linked with T2DM.30,31 This is in contrast to the result from another study showing the relation between lower educational level and high stress.32 Higher educational level is usually associated with higher responsibilities within the workstation and other additional responsibilities in the home and society. Therefore, this might have increased the stress level among the bank employees.
Study Highlights
What is current knowledge?
What is new here?
Conclusion
The findings of this study reveal that the majority of bank employees of Kathmandu Metropolitan City are living with the risk factors of T2DM. At least one risk factor was observed among all of the employees. The highest prevalence was the improper dietary habit followed by moderate to high levels of perceived stress and lack of sufficient physical activity. Risk factors like age, gender, level of education, marital status, socio-economic status, and family type were associated with the incidence of T2DM. Also, the study showed the urgent need to bring the attention of the concerned authorities to promote a healthy lifestyle, create a stress-free work environment, and awareness about the risk of T2DM among bankers, coming up with public health strategies for its prevention.
Acknowledgments
We would like to express our acknowledgment to all the participants of the study. Special thank goes to all the bank managers who allowed us to conduct this study.
Competing Interests
The authors declare that they have no competing interests.
Ethical Approval
The Institutional Review Committee, Manmohan Memorial Institute of Health Sciences, Kathmandu, Nepal reviewed and approved the study (registration number, MMIHS-IRC 468). Written informed consent was obtained from all the participants before the collection of data.
Supplementary Files
Supplementary file 1. Self-administered questionnaire.
(pdf)
References
- Lind M, Wedel H, Rosengren A. Excess mortality among persons with type 2 diabetes. N Engl J Med 2016; 374(8):788-9. doi: 10.1056/NEJMc1515130 [Crossref] [ Google Scholar]
- Salehidoost R, Mansouri A, Amini M, Aminorroaya Yamini S, Aminorroaya A. Diabetes and all-cause mortality, a 18-year follow-up study. Sci Rep 2020; 10(1):3183. doi: 10.1038/s41598-020-60142-y [Crossref] [ Google Scholar]
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019; 157:107843. doi: 10.1016/j.diabres.2019.107843 [Crossref] [ Google Scholar]
- Shrestha N, Mishra SR, Ghimire S, Gyawali B, Mehata S. Burden of diabetes and prediabetes in Nepal: a systematic review and meta-analysis. Diabetes Ther 2020; 11(9):1935-46. doi: 10.1007/s13300-020-00884-0 [Crossref] [ Google Scholar]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2006; 29 Suppl 1:S43-8. [ Google Scholar]
- Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab 2012; 37(3):540-2. doi: 10.1139/h2012-024 [Crossref] [ Google Scholar]
- Aravindalochanan V, Kumpatla S, Rengarajan M, Rajan R, Viswanathan V. Risk of diabetes in subjects with sedentary profession and the synergistic effect of positive family history of diabetes. Diabetes Technol Ther 2014; 16(1):26-32. doi: 10.1089/dia.2013.0140 [Crossref] [ Google Scholar]
- Jakes RW, Day NE, Khaw KT, Luben R, Oakes S, Welch A. Television viewing and low participation in vigorous recreation are independently associated with obesity and markers of cardiovascular disease risk: EPIC-Norfolk population-based study. Eur J Clin Nutr 2003; 57(9):1089-96. doi: 10.1038/sj.ejcn.1601648 [Crossref] [ Google Scholar]
- Manson JE, Greenland P, LaCroix AZ, Stefanick ML, Mouton CP, Oberman A. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. N Engl J Med 2002; 347(10):716-25. doi: 10.1056/NEJMoa021067 [Crossref] [ Google Scholar]
- Msopa E, Mwanakasale V. Identification of risk factors of diabetes mellitus in bank employees of selected banks in Ndola town. Diabetes Metab Syndr 2019; 13(2):1497-504. doi: 10.1016/j.dsx.2018.11.062 [Crossref] [ Google Scholar]
- Thapa S, Pyakurel P, Baral DD, Jha N. Health-related quality of life among people living with type 2 diabetes: a community based cross-sectional study in rural Nepal. BMC Public Health 2019; 19(1):1171. doi: 10.1186/s12889-019-7506-6 [Crossref] [ Google Scholar]
- Smriti Smriti, Rashmi A, Manjula A, Kurulkar PV, Kumar H. Assessment of risk factors for diabetes among bank employees using Indian diabetes risk score: a cross-sectional study. Indian J Public Health Res Dev 2020; 11(1):609-15. doi: 10.37506/ijphrd.v11i1.517 [Crossref] [ Google Scholar]
- Simkhada P, Poobalan A, Simkhada PP, Amalraj R, Aucott L. Knowledge, attitude, and prevalence of overweight and obesity among civil servants in Nepal. Asia Pac J Public Health 2011; 23(4):507-17. doi: 10.1177/1010539509348662 [Crossref] [ Google Scholar]
- Parashar P, Maroof KA, Bansal R, Ahmad S, Pant B. Prevalence and risk factors of diabetes among bank employees of Meerut district. Indian J Prev Soc Med 2009; 40(3):157-61. [ Google Scholar]
- Thapa S, Jha N, Baral DD, Pyakurel P. Health care seeking behaviour among people living with type-2 diabetes in rural area of eastern, Nepal. Int J Public Health Saf 2018; 3(3):166. [ Google Scholar]
- Dhimal M, Bista B, Bhattarai S, Dixit LP, Hyder M, Agarwal N, et al. Noncommunicable Disease Risk Factors: STEPS Survey Nepal 2019. Kathmandu: Nepal Health Research Council; 2020.
- Cohen S, Kamarck T, Mermelstein R. Perceived stress scale. In: Measuring Stress: A Guide for Health and Social Scientists. Vol 10. Oxford University Press; 1994. p. 1-2.
- Indian Council of Medical Research (ICMR), Public Health Foundation of India (PHFI), Institute for Health Metrics and Evaluation (IHME). Health of the Nation’s States: The India State-Level Disease Burden Initiative. New Delhi: ICMR, PHFI, IHME; 2017.
- Commar A, Vinayak P, d’Espaignet ET, Wolfenden L. WHO Global Report on Trends in Prevalence of Tobacco Use 2000-2025. 2nd ed. World Health Organization (WHO); 2018.
- Azimi-Nezhad M, Ghayour-Mobarhan M, Parizadeh MR, Safarian M, Esmaeili H, Parizadeh SM. Prevalence of type 2 diabetes mellitus in Iran and its relationship with gender, urbanisation, education, marital status and occupation. Singapore Med J 2008; 49(7):571-6. [ Google Scholar]
- Chang SA. Smoking and type 2 diabetes mellitus. Diabetes Metab J 2012; 36(6):399-403. doi: 10.4093/dmj.2012.36.6.399 [Crossref] [ Google Scholar]
- Thapa S, Kayastha P, Mishra DK. Assessment of risk of type 2 diabetes among adults of Banepa municipality, Nepal: community based cross-sectional study. Int J Travel Med Glob Health 2020; 8(1):31-6. doi: 10.34172/ijtmgh.2020.05 [Crossref] [ Google Scholar]
- Ely M, Hardy R, Longford NT, Wadsworth ME. Gender differences in the relationship between alcohol consumption and drink problems are largely accounted for by body water. Alcohol Alcohol 1999; 34(6):894-902. doi: 10.1093/alcalc/34.6.894 [Crossref] [ Google Scholar]
- Carlsson S, Hammar N, Grill V, Kaprio J. Alcohol consumption and the incidence of type 2 diabetes: a 20-year follow-up of the Finnish twin cohort study. Diabetes Care 2003; 26(10):2785-90. doi: 10.2337/diacare.26.10.2785 [Crossref] [ Google Scholar]
- Yuan S, Xue HL, Yu HJ, Huang Y, Tang BW, Yang XH. Cigarette smoking as a risk factor for type 2 diabetes in women compared with men: a systematic review and meta-analysis of prospective cohort studies. J Public Health (Oxf) 2019; 41(2):e169-76. doi: 10.1093/pubmed/fdy106 [Crossref] [ Google Scholar]
- Murakami K, Hashimoto H. Associations of education and income with heavy drinking and problem drinking among men: evidence from a population-based study in Japan. BMC Public Health 2019; 19(1):420. doi: 10.1186/s12889-019-6790-5 [Crossref] [ Google Scholar]
- Power C, Rodgers B, Hope S. Heavy alcohol consumption and marital status: disentangling the relationship in a national study of young adults. Addiction 1999; 94(10):1477-87. doi: 10.1046/j.1360-0443.1999.941014774.x [Crossref] [ Google Scholar]
- Liang W, Chikritzhs T. Brief report: marital status and alcohol consumption behaviours. J Subst Use 2012; 17(1):84-90. doi: 10.3109/14659891.2010.538463 [Crossref] [ Google Scholar]
- Salaroli LB, Saliba RA, Zandonade E, del Carmen Bisi Molina M, Bissoli NS. Prevalence of metabolic syndrome and related factors in bank employees according to different defining criteria, Vitória/ES, Brazil. Clinics (Sao Paulo) 2013; 68(1):69-74. doi: 10.6061/clinics/2013(01)oa11 [Crossref] [ Google Scholar]
- Lloyd C, Smith J, Weinger K. Stress and diabetes: a review of the links. Diabetes Spectr 2005; 18(2):121-7. doi: 10.2337/diaspect.18.2.121 [Crossref] [ Google Scholar]
- Kelly SJ, Ismail M. Stress and type 2 diabetes: a review of how stress contributes to the development of type 2 diabetes. Annu Rev Public Health 2015; 36:441-62. doi: 10.1146/annurev-publhealth-031914-122921 [Crossref] [ Google Scholar]
- Lunau T, Siegrist J, Dragano N, Wahrendorf M. The association between education and work stress: does the policy context matter?. PLoS One 2015; 10(3):e0121573. doi: 10.1371/journal.pone.0121573 [Crossref] [ Google Scholar]