J Res Clin Med. 13:34477.
doi: 10.34172/jrcm.025.34477
Short Communication
Investigating an unusual rise in blood-borne coagulase-negative Staphylococci in a tertiary health facility, Southwest Nigeria
Emmanuel Oladayo Irek Conceptualization, Data curation, Formal analysis, Methodology, Validation, Writing – original draft, Writing – review & editing, 1, 2, * 
Emmanuel Sunday Fajoyegbe Conceptualization, Validation, Writing – original draft, Writing – review & editing, 3
Odunayo Adebukola Temitope Fatunla Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 4
Adedayo Hakeem Oyebanji Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 4
Adekemi Kiyesi Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 5
Adeshola Adebayo Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 6
Anthony Chinemere Anuforo Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 7
Richmond Odele Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 8
Ezra Olatunde Ogundare Writing – original draft, Writing – review & editing, 9
Tosin Odunayo Babalola Validation, Writing – original draft, Writing – review & editing, 1
Temidayo Deborah Adebisi Validation, Writing – original draft, Writing – review & editing, 1
Josephine Chijioke Ihetu Writing – original draft, Writing – review & editing, 2
Mosunmola Margaret Fayomi Validation, Writing – original draft, Writing – review & editing, 2
Akinola Akimade Writing – original draft, Writing – review & editing, 10
Kolawole Olubunmi Ogundipe Writing – original draft, Writing – review & editing, 10
Author information:
1Department of Medical Microbiology and Parasitology, Afe Babalola University, Ado-Ekiti, Nigeria
2Department of Medical Microbiology and Parasitology, Afe Babalola Multi-System Hospital, Ado-Ekiti, Nigeria
3Department of Microbiology, Osun State University, Osogbo. Nigeria
4Department of Paediatrics, Afe Babalola Multi-System Hospital, Ado-Ekiti, Nigeria
5Department of Chemical Pathology, Afe Babalola Multi-System Hospital, Ado-Ekiti, Nigeria
6Department of Haematology, Afe Babalola Multi-System Hospital, Ado-Ekiti, Nigeria
7Department of Medical Microbiology and Parasitology, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria
8Department of Internal Medicine, Afe Babalola Multi-System Hospital, Ado-Ekiti, Nigeria
9Department of Paediatrics, Ekiti State University, Ado-Ekiti, Nigeria
10Department of Surgery, Afe Babalola University, Ado-Ekiti, Nigeria
Abstract
Introduction:
The clinical significance of coagulase-negative staphylococci (CoNS) is becoming increasingly concerning in healthcare settings, with dire consequences such as mortality. We investigated an unusual increase in blood-borne CoNS among patients in a private tertiary health facility in Southwest Nigeria and described mitigation strategies.
Methods:
CoNS bacteraemia descriptive analysis was conducted among inpatients between April 2022 and June 2022. Blood cultures were processed with an automated system. Phenotypic and molecular analyses (using 16S rDNA) of CoNS were performed according to established guidelines. We implemented the multimodal infection prevention and control (IPC) approach recommended by the World Health Organisation.
Results:
Eighty-two blood cultures (non-duplicate samples) were requested during the period. Of these, 30 (36.5%) were culture-positive, and 10 were CoNS (10/30, 33.3%).The cumulative incidence of CoNS bacteraemia was 12 cases per 100 patients over 90 days, compared to 1-2% in previous months. Staphylococcus haemolyticus (4/10, 40%), Staphylococcus hominis (3/10, 30%), Staphylococcus epidermidis (2/10, 20%), and Staphylococcus saccharolyticus (1/10, 10%) were identified. All isolates were resistant to ciprofloxacin, trimethoprim-sulfamethoxazole, and cefoxitin (methicillin-resistant surrogate marker), while they were susceptible to vancomycin and linezolid. All the isolates fell into the S. epidermidis and S. haemolyticus clusters in phylogenetic studies. The rates returned to baseline following the implementation of the IPC strategies.
Conclusion:
The unusual surge in CoNS incidence at the hospital resulted from multidrug-resistant clusters of S. haemolyticus and S. epidermidis, which were addressed by the implementation of multimodal IPC strategies.
Keywords: Cross-infection, Infection control, Nigeria, Sepsis
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
Afe Babalola Multi-System Hospital, Ado-Ekiti, funded a part of the molecular analysis.
Introduction
Coagulase-negative staphylococci (CoNS) are increasingly recognised as bacteria of true clinical significance.1-3 Determining the clinical importance of CoNS as blood-borne pathogens can be difficult due to the prevailing perception of them as skin flora contaminants.1,4 CoNS comprise a heterogeneous group of staphylococci, with Staphylococcus epidermidis recognised as one of the most notorious pathogens, particularly in patients with invasive medical devices, implants, or prostheses.1 However, within this group, there appears to be a competing rise of other staphylococci such as Staphylococcus haemolyticus and Staphylococcus hominis within the clusters of S. epidermidis and S. haemolyticus in clinical settings.5,6 The clinical relevance of CoNS in hospital environments is attributed to their niche on human skin, which grants them access to any inserted devices. Additionally, their ability to form biofilms on devices by producing capsular polysaccharide adhesin, along with the increasing use of prosthetic devices among immunocompromised patients, renders them formidable pathogens. 1,5 Furthermore, most healthcare-acquired CoNS harbour antibiotic-resistance genes, complicating management of infected patients.1 This issue is particularly prevalent in settings with weak infection prevention and control (IPC) practices, where the multimodal IPC strategy of the World Health Organization (WHO) is often not implemented.7 Accurate speciation of CoNS using conventional biochemical methods is challenging, which may downplay the clinical relevance of species. The incidence of CoNS varies across Africa in humans and animals (mainly cattle), ranging from 6% to 68% in suspected human infections and 3% to 61.7% in suspected animal infections, distributed across different geographic locations. However, little is known about the diversity and characterization of blood-borne CoNS in clinical settings in Nigeria.8 We investigated an unusual surge in the incidence of CoNS bacteraemia among inpatients in a private tertiary hospital in Southwest Nigeria, applying the WHO multimodal IPC strategies to control these infections.
Methods
Patients’ characteristics
A retrospective analysis was conducted from April 2022 to June 2022 among inpatients at a private tertiary hospital with suspected bloodstream infection (BSI). All data were collected by reviewing the electronic medical records of CoNS bacteraemia cases during the study period, using laboratory surveillance corroborated by clinical suspicion of bloodstream infection. For patients suspected of having BSI, at least one set of blood cultures consisting of two automated culture bottles was collected within 24 hours of the suspicion of bloodstream infection, using povidone-iodine and 70% methylated spirit as skin antiseptics.9 Patients were deemed to have a bloodstream infection when presenting with a temperature of ≥ 38 °C or < 36 °C and other systemic signs of infection, accompanied by one or more positive blood cultures.10 Organ failure following a bloodstream infection was assessed using the Sequential Organ Failure Assessment Score (SOFA).11 Scores were incrementally assigned based on the increasing severity of the parameters outlined, with a maximum of 24. SOFA scores include parameters that assess the severity of several body systems: respiratory (lung function), cardiovascular (heart function and need for vasopressors), coagulation (platelet count), central nervous system (Glasgow Coma Scale), renal (creatinine assay/urine output), and liver function (bilirubin assay).12 Blood sampling from patients with invasive intravascular catheters was performed following standard guidelines.13 A true pathogen from blood culture was identified when at least two bottles obtained from the patient were positive for the same organism within 48 hours of incubation.9
Phenotypic characterisation of bacteria
Blood culture bottles were processed in an automated blood culture system (TDR–X030, Mindray, Nanshan, China). Upon receiving a positive signal, the blood specimens were subcultured onto 5% sheep blood agar and MacConkey agar plates. These plates were incubated for 18 to 24 hours at 35 ± 2 ºC. Gram staining was performed on the culture colonies followed by catalase and coagulase tests on the Gram-positive cocci isolates, which were subcultured onto Mannitol salt agar to identify CoNS further. Antimicrobial susceptibility testing was performed using the Modified Kirby-Bauer disc diffusion method, following Clinical and Laboratory Standards Institute (CLSI) guidelines.14 Staphylococcus aureus ATCC® 25923 was used as a positive control. The following antibiotics (Mast®, United Kingdom) were used for susceptibility testing: Cefoxitin 30 µg, gentamicin 10 µg, amikacin 30 µg, erythromycin 15 µg, ciprofloxacin 5 µg, clindamycin 2 µg, trimethoprim-sulfamethoxazole 1.25/23.75 µg, chloramphenicol 30 µg, rifampicin 5 µg, and linezolid 30 µg. The estimation of vancomycin minimum inhibitory concentration (MIC) with MIC test strip (Liofilchem®, Italy) was conducted and interpreted using the CLSI guidelines.14
Molecular characterisation of bacteria
Molecular identification using 16S rDNA was performed for the CoNS isolates. Genomic DNA was extracted with a Quick-DNA Bacterial Miniprep Kit (Zymo Research, Catalogue No. D6005). The 16S rRNA region was amplified using universal 16s rRNA primers. PCR amplification was performed in a total reaction volume of 25 µL, which included 0.5 µL each of the 27F and 1492R universal 16s rDNA primers (Liao et al., 2016), 12.5 µL of OneTaq Quick-Load 2X Master Mix with Standard Buffer (NEB, England), 2 µL of template DNA, and 9.5 µL of nuclease-free water. The 5’-3’ sequences of the universal primers used were 16s-27f, AGAGTTTGATCMTGGCTCAG and 16s-1492r, CGGTTACCTTGTTACGACTT. PCR amplification of the 16S rRNA gene of interest was conducted in a Mastercycler nexus gradient (Eppendorf, Germany), starting with an initial denaturation at 94 °C for 5 minutes, followed by 35 cycles of denaturation at 94 °C for 30 seconds, annealing at 50 °C for 30 seconds, and extension at 68 °C for 1 minute and 30 seconds, concluding with a final extension at 68 °C for 10 minutes. The PCR products were electrophoresed on a 1% agarose gel, stained with Safeview, and visualised using a gel documentation system (E-BOX, Vilber Lourmat, Italy). PCR amplification using the primer set of universal 16s rRNA primers yielded a single amplicon of 1500 bp in all strains.
The PCR products were gel-extracted using the ZymocleanTM Gel DNA Recovery Kit (Zymo Research, Catalogue No. D4001). The extracted fragments were sequenced in the forward and reverse direction using a Brilliant Dye Terminator Cycle Sequencing Kit (Nimagen, Brilliant Dye Terminator Cycle Sequencing Kit V3.1, BRD3100/1000) and purified (Zymo Research, Catalogue No. D4050). The purified fragments were loaded and analysed on the ABI 3500XL Genetic Analyser (Applied Biosystems, Thermo Fisher Scientific) for each reaction, and the sequenced data were collected. CLC Bio Main Workbench v7.6 was used to analyse the files generated by the ABI3500XL. The trimmed data were submitted to Blastn on NCBI to identify close sequence matches (http://www.ncbi.nlm.nib.gov/BLAST/blast). Nucleotide sequences determined in this study were submitted to the GenBank database with accession numbers PP758173-PP758178 for the identified CoNS.
A phylogenetic analysis was also performed on the CoNS isolates using Molecular Evolutionary Genetic Analysis (MEGA®) version 11 to determine genetic relatedness. The maximum likelihood method and the Tamura-Nei model were used to infer evolutionary history. The bootstrap consensus tree inferred from 1000 replicates was taken to represent the evolutionary history of the analysed taxa. Branches corresponding to partitions reproduced in less than 50% of bootstrap replicates were collapsed. The percentage of replicate trees in which the associated taxa clustered together in the bootstrap test of 1000 replicates is shown next to the branches. Initial tree(s) for the heuristic search were automatically obtained by applying Neighbour-Join and BioNJ algorithms to a matrix of pairwise distances estimated using the Tamura-Nei model and then selecting the topology with the superior log-likelihood value.16
Statistical analysis
Univariate statistical analysis was conducted and presented as frequency distribution, percentages, means and standard deviation. Adjusted odds ratios were estimated to assess the strength associations, and 95% confidence interval was used to test for analytical significance.
Results
Patients’ characteristics
Eighty-two blood cultures (non-duplicate samples) were requested for patients suspected of BSI between April and June 30, 2022. Of these, 30 (36.5%) were positive for an organism, while 10 of the positive blood cultures were CoNS (10/30, 33.3%). A blood contamination rate of 3.3% (1/30) was noted during the same period.
The CoNS identified in decreasing order were Staphylococcus haemolyticus (4/10, 40%), Staphylococcus hominis (3/10, 30%), Staphylococcus epidermidis (2/10, 20%), and Staphylococcus saccharolyticus (1/10, 10%) (Table 1).
Table 1.
The characteristics of the 10 patients identified with CoNS bacteraemia in the health facility
|
Patients’ ID
|
Organism identified
|
Initial diagnosis
|
Age (years)
|
SOFA score as at BSI
|
Blood culture Time to positivity (hours)
|
Ward of admission at BSI
|
Admitted day (s) to BSI
|
Central line inserted
|
Hospitalization length (days)
|
Outcome
|
| Abuad 1 |
Staphylococcus haemolyticus
|
Severe head trauma |
24 |
15 |
24 |
ICU |
21 |
yes |
17 |
In-hospital mortality |
| Abuad 2 |
Staphylococcus haemolyticus
|
Severe head trauma |
81 |
15 |
36 |
ICU |
44 |
yes |
50 |
In-hospital mortality |
| Abuad 3 |
Staphylococcus hominis
|
Type 2DM and CKI |
71 |
10 |
48 |
Renal |
3 |
yes |
5 |
In-hospital mortality |
| Abuad 4 |
Staphylococcus haemolyticus
|
Type 2DM and Hypertension |
55 |
6 |
24 |
ICU |
4 |
yes |
40 |
In-hospital mortality |
| Abuad 5 |
Staphylococcus saccharolyticus
|
Neonatal sepsisa |
1 week |
5 |
24 |
SCBU |
5 |
no |
10 |
Discharged alive |
| Abuad 6 |
Staphylococcus hominis
|
Hypertension |
35 |
1 |
48 |
ER |
1 |
no |
6 |
Discharged alive |
| Abuad 7 |
Staphylococcus epidermidis
|
Hepatitis B & ESRD |
38 |
6 |
48 |
Renal |
3 |
yes |
8 |
Discharged alive |
| Abuad 8 |
Staphylococcus haemolyticus
|
Severe head trauma |
42 |
7 |
24 |
ICU |
3 |
yes |
40 |
Discharged alive |
| Abuad 9 |
Staphylococcus hominis
|
Neonatal sepsisa |
1 week |
5 |
36 |
SCBU |
2 |
no |
10 |
Discharged alive |
| Abuad 10 |
Staphylococcus epidermidis
|
Gastroenteritis and chronic Lymphoedema |
48 |
2 |
24 |
FSW |
3 |
yes |
8 |
Discharged alive |
SOFA, Sequential [Sepsis-Related] Organ Failure Assessment Score; FSW, Female surgical ward; SCBU, Special care baby unit; CKI, chronic kidney injury; ESRD, End stage renal disease; ER, Emergency room.
aLikely diagnosis.
Patients with a mean SOFA score of 11.5 (SD ± 4.3) had adjusted odds of 1.45 (95% CI 2.33-11.99) of dying with CoNS bacteraemia. All patients had one or more devices used during their hospital stay, such as an indwelling catheter or peripheral intravenous cannula, while 70% (7/10) of the patients had a central venous catheter inserted for various medical or surgical indications. The calculated cumulative incidence of CoNS bacteraemia in the hospital was 12 cases per 100 patients over the 90-day investigation, compared to a sporadic occurrence of 1-2 cases per 100 patients over the previous 90 days. The incidence density was 11.5 per 100 patient-days of admission during this period.
The application of the multimodal strategic IPC approach reduced the bloodstream isolation of CoNS to a baseline of 3 cases per 100 patients over the next three months. This was achieved through a stepwise implementation of system changes, education, awareness-raising, monitoring, and sustained surveillance.
Antibiotic susceptibility profile of CoNS
The antibiogram shown in Table 2 displays the multi-drug resistance profiles of the CoNS identified with 12 antibiotics. There was 100% resistance to Trimethoprim-sulfamethoxazole and ciprofloxacin, and all the CoNS were methicillin-resistant; as determined using cefoxitin 30 µg disc as a surrogate marker. Antibiotic resistance was high, following this order: gentamicin > chloramphenicol > tetracycline > clindamycin. All isolates were susceptible to both vancomycin and linezolid, while amikacin and rifampicin had the lowest antibiotic resistance rates of 10% and 20%, respectively. Sixty percent (6/10) of the CoNS were D-test positive, serving as a surrogate marker for inducible clindamycin resistance mediated by the erm gene.
Table 2.
The antimicrobial susceptibility profile of CoNS in the private tertiary health facility describing the phenotypic characterization
|
Antimicrobial agent
|
Percentage of CoNS
|
|
Susceptible
|
Intermediate
|
Resistant
|
| Azithromycin |
30 |
10 |
60 |
| Gentamicin |
20 |
0 |
80 |
| Amikacin |
90 |
0 |
10 |
| Ciprofloxacin |
0 |
0 |
100 |
| Cefoxitin |
0 |
0 |
10 |
| Clindamycin |
30 |
10 |
60 |
| Linezolid |
100 |
0 |
0 |
| Tetracycline |
40 |
0 |
60 |
| Trimethoprim-sulfamethoxazole |
0 |
0 |
100 |
| Chloramphenicol |
30 |
0 |
70 |
| Rifampicin |
80 |
0 |
20 |
| Vancomycin |
100 |
0 |
0 |
Molecular characterization
Abuads 1, 2, 4, and 8 shared a common ancestor and grouped into a monophyletic clade named ICU Clade, which comprises only Staphylococcus haemolyticus strains. Abuads 5, 7, and 10 were also closely related, culminating in another clade. The last clade consisted of a distantly related ER (Abuad 6) strain and another SCBU strain (Abuad 9), both identified as Staphylococcus hominis. The outlier (Staphylococcus hominis) was from the renal ward (Figure 1).
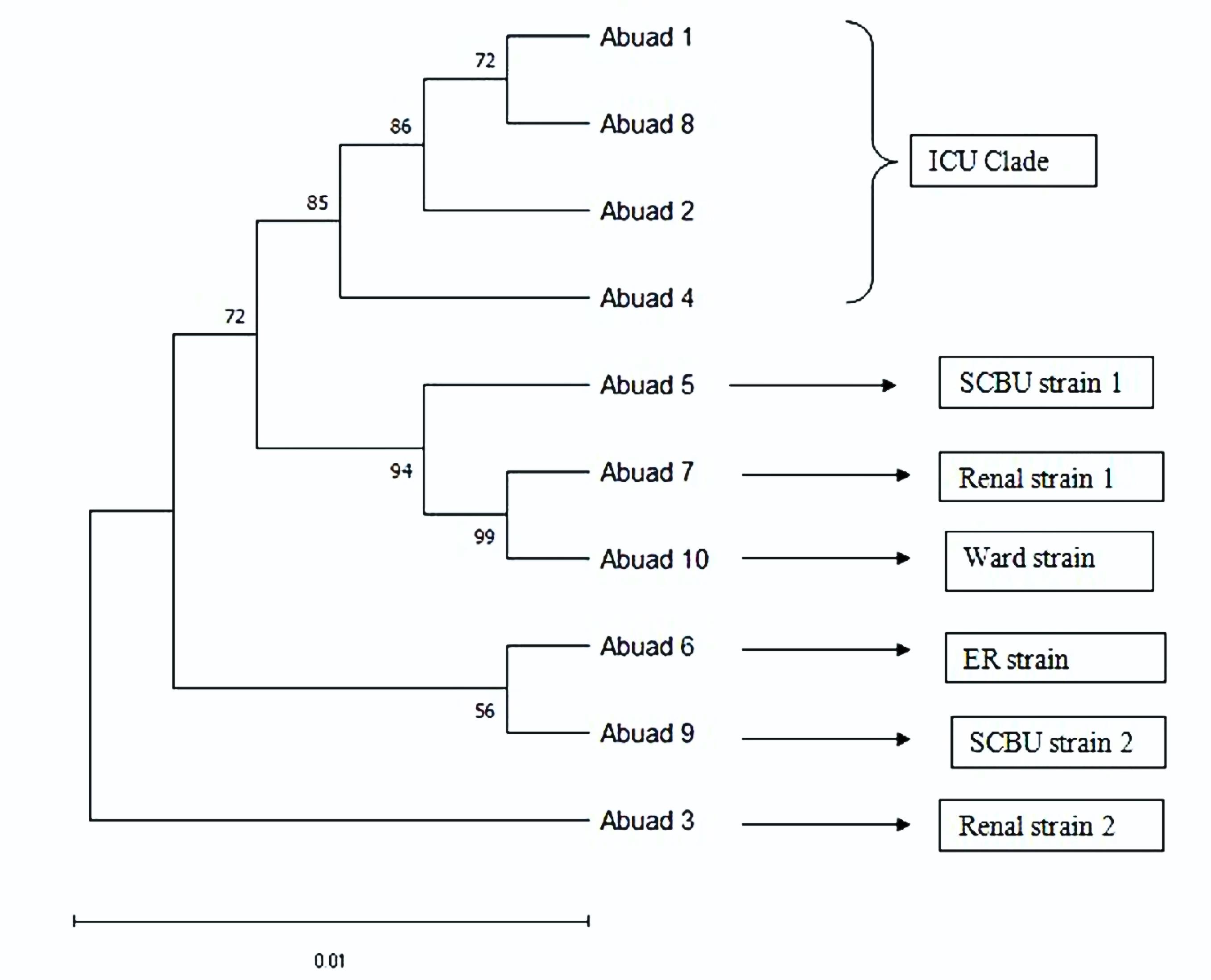
Figure 1.
The phylogenetic relationship between the strains of the CoNS identified
.
The phylogenetic relationship between the strains of the CoNS identified
Discussion
Patients’ management
The earliest indication of an unusual surge in CoNS incidence, based on laboratory surveillance, was identified in patients admitted to the intensive care unit (ICU). Subsequent identifications occurred in other wards within the health facility. Until then, only sporadic cases of CoNS had been observed in blood culture samples at the health facility. Most of these affected patients were located in high-dependency wards (such as the SCBU and renal-transplant ward) and the ICU, which directly or indirectly facilitates the emergence of ‘super-bugs’. It is known that the intensive care unit serves as a breeding ground for antimicrobial-resistant organisms due to the extensive use of antibiotics, the use of numerous invasive devices, and the characteristics of the vulnerable population present. However, the identification of CoNS bacteraemia was unexpected since it is primarily considered a normal flora of the skin and a probable contaminant of blood culture. Its role as a true pathogen was supported by the significantly increased morbidity during the bacteraemic episodes, as shown by SOFA11 and laboratory analysis.9
Although CoNS bacteraemia has been identified in Nigeria,18 its epidemiology and molecular characterization have not been fully elucidated despite its notoriety for nosocomial bacteraemia in other regions.19 The culture positivity rate of CoNS in the study was within the range of 5- 39.6%,20,21 consistent with the rates found in most identified CoNS bacteraemia cases. Most studies on CoNS identify invasive devices as risk factors for bacteraemia, which aligns with our findings, as all the patients had one or more devices during their bacteraemia episodes (Table 1). Approximately three-quarters of the patients underwent invasive intravascular catheterization, potentially predisposing them to CoNS bacteraemia. The molecular analysis revealed a diversity of CoNS observed during this period (Figure 1), explaining the heterogeneity and virulence of emerging CoNS in this environment. This contrasts with the usual preponderance of S. epidermidis in bloodstream infections.18,22 The clonal distribution of these CoNS confirmed the suspicion of a potential ongoing ICU clustering of CoNS, albeit with varying degrees of homology. The ICU clade falls within the S. haemolyticus cluster and the S. epidermidis-aureus species group,6 while the other strains identified in the health facility during this period cluster within S. epidermidis and S. haemolyticus. Based on this study, these cluster groups are predominant CoNS in the health facility and appear to be emerging clusters, particularly given the associated antibiotic resistance.23
The extensive antibiotic resistance patterns observed in CoNS in this study (Table 2) were consistent with reports from other countries.24 Vancomycin (a glycopeptide) and linezolid (an oxazolidinone) exhibited the best susceptibility profile; however, their use may have been hindered by inaccessibility and unavailability at the time of this investigation. These antibiotics have shown clinical efficacy in many cases of CoNS bacteraemia, especially those involving methicillin resistance, which was predominant in this study.13 The widespread antibiotic resistance identified in this study further limited the clinical management of the patients.
Therefore, identifying blood-borne CoNS in patients should heighten clinical suspicion of potential pathogenicity rather than merely indicating contamination, especially in high-dependency wards or ICUS. This study has some limitations, as the eventual mortality of certain infected patients cannot be entirely attributed to the acquisition of CoNS.
Application of the WHO multimodal strategic approach
Recognizing the significant reduction of healthcare-associated infections achieved with the WHO multimodal IPC approach,7 the infection prevention and control team of the health facility recommended 2% chlorhexidine gluconate as skin antisepsis during the insertion of invasive vascular devices (peripheral and central lines) as a form of systemic change. The wards where the CoNS were identified were decontaminated with a formaldehyde-based solution, recognising the environmental reservoir as a potential source of CoNS on inanimate objects. Subsequently, staff in the affected wards were required to adhere to standard precautions, especially hand hygiene.7,25,26 Monitoring and evaluation were conducted by the supervising heads of the respective wards and units, while feedback was passed on to the infection prevention team for further action. Visible reminders and awareness displays had already been established in many areas of the hospital. There was initial resistance to this approach from healthcare workers due to understaffing and high patient volume, which was thoroughly discussed for action. Surveillance was maintained by the infection prevention team through laboratory surveillance. The reduction in bloodstream CoNS isolation confirmed the effectiveness of the IPC strategy.7
Conclusion
The unusual rise in CoNS incidence at the hospital was caused by multidrug-resistant clusters of S. haemolyticus and S. epidermidis. This was mitigated through the implementation of IPC multimodal strategies.
Competing Interests
The authors declare that they have no competing interests
Ethical Approval
This study was a retrospective analysis that included a waiver of formal consent and patient details. Relevant information was collected by reviewing the electronic medical records of all cases of CoNS bacteraemia during the study period. The ethics review committee of the health facility approved this study, with approval number AMSH/REC/IEO/128.
Acknowledgements
We sincerely appreciate Mr. Emmanuel I. Durojaye, Mr. Bodunwa Kayode, and the other support staff from both the Department of Medical Microbiology and Parasitology at Afe Babalola University and Afe Babalola Multi-System Hospital. I am grateful to the Nigeria Field Epidemiology and Laboratory Programme, Abuja, for their intellectual support.
References
- Rupp ME, Fey PD. Staphylococcus epidermidis and other coagulase-negative staphylococci. In: Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 9th ed. Elsevier; 2020. p. 2432-43.
- Becker K, Harmsen D, Mellmann A, Meier C, Schumann P, Peters G. Development and evaluation of a quality-controlled ribosomal sequence database for 16S ribosomal DNA-based identification of Staphylococcus species. J Clin Microbiol 2004; 42(11):4988-95. doi: 10.1128/jcm.42.11.4988-4995.2004 [Crossref] [ Google Scholar]
- Toltzis P. Staphylococcus epidermidis and other coagulase-negative staphylococci. In: Principles and Practice of Pediatric Infectious Diseases. 5th ed. Springer International Publishing; 2018. p. 706-12.
- Kim J, Hong J, Lim JA, Heu S, Roh E. Improved multiplex PCR primers for rapid identification of coagulase-negative staphylococci. Arch Microbiol 2018; 200(1):73-83. doi: 10.1007/s00203-017-1415-9 [Crossref] [ Google Scholar]
- Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev 2014; 27(4):870-926. doi: 10.1128/cmr.00109-13 [Crossref] [ Google Scholar]
- Lamers RP, Muthukrishnan G, Castoe TA, Tafur S, Cole AM, Parkinson CL. Phylogenetic relationships among Staphylococcus species and refinement of cluster groups based on multilocus data. BMC Evol Biol 2012; 12:171. doi: 10.1186/1471-2148-12-171 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Guidelines on Core Components of Infection Prevention and Control Programmes at the National and Acute Health Care Facility Level. Geneva: WHO; 2016. Available from: https://www.who.int/publications/i/item/9789241549929.
- Asante J, Amoako DG, Abia AL, Somboro AM, Govinden U, Bester LA. Review of clinically and epidemiologically relevant coagulase-negative staphylococci in Africa. Microb Drug Resist 2020; 26(8):951-70. doi: 10.1089/mdr.2019.0381 [Crossref] [ Google Scholar]
- Wilson ML, Weinstein MP, Reller LB. Laboratory detection of bacteremia and fungemia. In: Manual of Clinical Microbiology. 11th ed. ASM; 2015. p. 15.
- Lutwick L, Bearman G. Bloodstream infections. In: Guide to Infection Control in the Hospital. 5th ed. ISID; 2018. p. 410.
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016; 315(8):801-10. doi: 10.1001/jama.2016.0287 [Crossref] [ Google Scholar]
- United Kingdom Sepsis Trust. The Sepsis Manual. 6th ed. United Kingdom Sepsis Trust; 2022. p. 19-20.
- Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O’Grady NP. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis 2009; 49(1):1-45. doi: 10.1086/599376 [Crossref] [ Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 31st ed. CLSI Supplement M100. CLSI; 2021.
- Lane DJ. 16S/23S rRNA sequencing. In: Stackebrandt E, Goodfellow M, eds. Nucleic Acid Techniques in Bacterial Systematics. Chichester: John Wiley & Sons; 1991. p. 115-75.
- Tamura K, Stecher G, Kumar S. MEGA11: molecular evolutionary genetics analysis version 11. Mol Biol Evol 2021; 38(7):3022-7. doi: 10.1093/molbev/msab120 [Crossref] [ Google Scholar]
- Brusselaers N, Vogelaers D, Blot S. The rising problem of antimicrobial resistance in the intensive care unit. Ann Intensive Care 2011; 1:47. doi: 10.1186/2110-5820-1-47 [Crossref] [ Google Scholar]
- Grace JU, Olayinka BO, Onaolapo JA, Obaro SK. Staphylococcus aureus and coagulase-negative staphylococci in bacteraemia: the epidemiology, predisposing factors, pathogenicity and antimicrobial resistance. Clin Microbiol 2019; 8(2):325. doi: 10.4172/2327-5073.1000325 [Crossref] [ Google Scholar]
- Hurley JC. Incidence of coagulase-negative staphylococcal bacteremia among ICU patients: decontamination studies as a natural experiment. Eur J Clin Microbiol Infect Dis 2020; 39(4):657-64. doi: 10.1007/s10096-019-03763-0 [Crossref] [ Google Scholar]
- Tashiro M, Izumikawa K, Ashizawa N, Narukawa M, Yamamoto Y. Clinical significance of methicillin-resistant coagulase-negative staphylococci obtained from sterile specimens. Diagn Microbiol Infect Dis 2015; 81(1):71-5. doi: 10.1016/j.diagmicrobio.2014.09.019 [Crossref] [ Google Scholar]
- Asaad AM, Qureshi MA, Hasan SM. Clinical significance of coagulase-negative staphylococci isolates from nosocomial bloodstream infections. Infect Dis (Lond) 2016; 48(5):356-60. doi: 10.3109/23744235.2015.1122833 [Crossref] [ Google Scholar]
- Yamada K, Namikawa H, Fujimoto H, Nakaie K, Takizawa E, Okada Y. Clinical characteristics of methicillin-resistant coagulase-negative staphylococcal bacteremia in a tertiary hospital. Intern Med 2017; 56(7):781-5. doi: 10.2169/internalmedicine.56.7715 [Crossref] [ Google Scholar]
- Cui J, Liang Z, Mo Z, Zhang J. The species distribution, antimicrobial resistance and risk factors for poor outcome of coagulase-negative staphylococci bacteraemia in China. Antimicrob Resist Infect Control 2019; 8:65. doi: 10.1186/s13756-019-0523-5 [Crossref] [ Google Scholar]
- Bhatt P, Tandel K, Singh A, Kumar M, Grover N, Sahni AK. Prevalence and molecular characterization of methicillin resistance among coagulase-negative staphylococci at a tertiary care center. Med J Armed Forces India 2016; 72(Suppl 1):S54-8. doi: 10.1016/j.mjafi.2016.03.007 [Crossref] [ Google Scholar]
- Marchant EA, Boyce GK, Sadarangani M, Lavoie PM. Neonatal sepsis due to coagulase-negative staphylococci. Clin Dev Immunol 2013; 2013:586076. doi: 10.1155/2013/586076 [Crossref] [ Google Scholar]
- Qazi SA, Stoll BJ. Neonatal sepsis: a major global public health challenge. Pediatr Infect Dis J 2009; 28(1 Suppl):S1-2. doi: 10.1097/INF.0b013e31819587a9 [Crossref] [ Google Scholar]