J Res Clin Med. 13:33468.
doi: 10.34172/jrcm.025.33468
Original Article
Peer support as a preventive intervention for postpartum anxiety: A single-blind randomized clinical trial
Mahin Kamalifard Conceptualization, Investigation, Methodology, Project administration, Validation, Writing – review & editing, 1 
Rogayyeh Iraji-Iranagh Resources, Writing – original draft, Writing – review & editing, 1, *
Parisa Yavarikia Supervision, Visualization, Writing – review & editing, 1
Jalil Babapour-Kheiroddin Data curation, Formal analysis, Software, Writing – review & editing, 2
Author information:
1Department of Midwifery, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran
2Department of Psychology, Faculty of Educational Sciences and Psychology, Tabriz University, Tabriz, Iran
Abstract
Introduction:
This study aimed to evaluate the effects of peer support on postpartum anxiety and self-esteem among first-time mothers (primiparous women) referred to health centers.
Methods:
A total of 100 eligible primiparous women were randomly assigned to two groups: the intervention group, which received standard care along with peer support, and the control group, which received only routine care. To ensure blinding and concealment of allocation, the randomization sequence was managed by an individual not involved in participant recruitment or data collection. Peer supporters were instructed to contact the mothers they were supporting at least once a week. The effectiveness of the peer support intervention was assessed by administering the Rosenberg Self-Esteem Scale and the Spielberger Anxiety Inventory to all participants before and after the intervention.
Results:
The intervention group exhibited a significantly lower mean state anxiety score compared to the control group (P=0.023). However, there was no statistically significant difference observed in trait anxiety (P=0.162) or the timing of first breastfeeding (P=0.037). Notably, the intervention group demonstrated a higher rate of breastfeeding continuation at two months postpartum.
Conclusion:
The findings suggest that incorporating peer support into standard prenatal care can be beneficial in reducing postpartum anxiety among first-time mothers. It is recommended that healthcare providers consider integrating peer support mechanisms into their routine maternal care practices.
Keywords: Anxiety, Peer group, Postpartum
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This study was funded by Tabriz University of Medical Sciences.
Introduction
The journey into motherhood begins with pregnancy and the anticipation of childbirth, marking a significant change in a woman’s life.1 This transition is not just a passive experience; it involves active changes in roles and identities for both parents.2 During this crucial time, mothers need to develop various skills and knowledge that will impact the health and well-being of their newborns.3 Nulliparous, face unique challenges compared to those who have given birth before. Research shows that they often experience higher levels of fear, anxiety, and lower self-esteem regarding their ability to care for a newborn. These psychological challenges can lead to difficulties in forming emotional bonds with their babies and may affect breastfeeding success. According to comprehensive analyses, the pooled prevalence rates for various forms of anxiety are calculated to be approximately 4% for generalized anxiety disorder, 15% for anxiety specifically related to pregnancy and an alarming 23% when employing established cut-off scores on validated self-report questionnaires that assess anxiety levels.4 Anxiety during pregnancy can have serious consequences, including complications like preterm labor and low birth weight, reduced head circumference, exacerbation of hyperemesis symptoms, an increased likelihood of postpartum mood disorders, and a greater propensity for behaviors such as cigarette and alcohol consumption, all of which can adversely affect the developing infant and the mother-infant relationship, as well as impair the mother’s ability to engage in successful breastfeeding practices. Moreover, severe and persistent levels of maternal anxiety have been shown to lead to an increase in serum glucocorticoid levels, which is consequent to the induction of significant neuroendocrine changes; these changes, in turn, are associated with cognitive or behavioral problems that manifest during both the prenatal period and throughout early childhood development.5 It can also lead to postpartum mood disorders and affect the mother-infant relationship. Studies indicate that a significant percentage of pregnant women experience anxiety, which can have lasting effects on both the mother and child.6 Building a strong emotional connection between mother and child is essential for successful breastfeeding.7,8 Primiparous often seek support from other women who are also navigating motherhood. These connections provide valuable social support, helping to reduce anxiety and improve self-esteem.8,9 Support groups formed during prenatal classes can help address the needs of mothers in the postpartum period. These groups foster community and provide a space for sharing experiences, which can enhance health awareness and promote positive behaviors.10-12 This study aims to explore the effects of peer support on postpartum anxiety and self-esteem among first-time mothers, considering the specific cultural context of our community.
Materials and Methods
Study design and participants
This single-blind randomized clinical trial is a part of a previously published study.13 It was meticulously conducted in 2012 with the aim of evaluating the impact of peer support on anxiety levels (primary outcome), alongside self-esteem and the sustained practice of breastfeeding (secondary outcome) among women who were referred to health centers.
The study population consisted of primiparous pregnant women who received telephone support from peer counselors starting from the last trimester of their gestation period and extending until two months post-delivery. Additional eligibility criteria encompassed being the ages of 18 to 35 years, with no underlying medical conditions such as diabetes mellitus, epilepsy, hypertension, anemia, and hypothyroidism. Participants also should not have experienced adverse life events within the preceding six months. The fetus; health was confirmed by ultrasound, and participants were not taking psychotropic medications or diagnosed with psychotic or bipolar disorders
Sample size
G-Power statistical software was used to calculate the required sample size, considering a 15% reduction in average anxiety score, based on data from Shahhosseini and colleagues’ research.14 The total sample size was 40 women, accounting for a 10% attrition rate. The expected number of samples for each group was 45 individuals, but with a 10% probability of participant loss, the final calculation yielded 50 individuals for each group.
Sampling
Following the acquisition of approval from the regional ethics committee, as well as the formal registration of the study, a total of 20 public healthcare centers in Tabriz that demonstrated the highest referral rates for pregnant women were meticulously selected. To facilitate this selection, a comprehensive inventory of health centers was compiled, leading to the identification of those facilities that attracted the most clients seeking prenatal care services. The sampling process commenced at the center with the highest volume of activity and continued systematically until the requisite sample size was achieved. All participants were required to sign a written informed consent document before their inclusion in the study.
Randomization and intervention
The women who were recruited were subjected to random assignment into two distinct groups: (Group 1: intervention) peer support + standard care protocols; and (Group 2: control) only the standard care protocols.
The allocation sequence was determined using a computer-generated randomization protocol, with a 1:1 allocation ratio, and an individual not involved in participant recruitment or data collection was responsible.
The participants possessed experience in both delivery methods (Cesarean section or normal vaginal delivery) and breastfeeding and were proficient in reading and writing in Persian. Seventeen peer mothers who were already seeking help at health centers were chosen to participate in the study. After they agreed to be part of the research, they attended two days of 4-hour training sessions. During these sessions, the peers discussed the implementation of the intervention and shared information regarding various issues and challenges encountered during pregnancy and the postpartum period; additionally, a comprehensive 10-page manual was provided to each participant. The peer mothers were asked to call each mother they were helping at least once a week. They were supposed to offer emotional support and share their own experiences with pregnancy, childbirth, and the postpartum period. The peer mothers were given a guide and a form to keep track of their calls, including how long they talked, what they discussed, and the results of the conversations. These records were then sent to the researcher.
Following interviews that verified their competencies as supportive counterparts, the mothers were assured of the confidentiality of their information. Furthermore, all expenses associated with telephone calls and travel to designated centers were borne by the researcher.
On average, peer telephone calls commenced within one week following randomization. Mothers in the control group received regular prenatal and postnatal care from health centers. Mothers in the intervention group also received regular care, but they additionally received support and guidance from other mothers (peers).
Peers provided with the researcher’s contact information were empowered to reach out to the researcher in the event of issues or for further clarification. Additionally, the telephone counterparts were contacted every week to monitor the progress of the intervention. A call registration form was provided to the peers to document the time, date, and duration of each call, which was to be submitted to the researcher after the study. In order to mitigate the risk of peers becoming familiar with the participating mothers and thereby compromising the confidentiality of personal information, the peers were selected from different health centers than those frequented by the mothers involved in the study. The primary outcome measured was Postpartum Anxiety, while secondary outcomes included self-esteem and breastfeeding practices.
Data collection tools
The data collection tools encompassed socio-demographic information about the mothers, which included variables such as age, occupation, education level, and the extent of social and emotional support received from their spouses and families. The other data collection tool included midwifery and postpartum information (gestational age at delivery, type of delivery, infant gender, birth weight, Apgar score, birth defects, hospitalization, infant weight at two months, time of first breastfeeding, and continuity of breastfeeding at two months), Spielberger Anxiety Questionnaire, and Rosenberg Self-Esteem Scale.
The Spielberger Anxiety Inventory consists of 40 items, 20 items related to state anxiety, based on the answer given (not at all, low, high, and very high), a score of one to four is assigned to each item.
The other 20 phrases are related to latent anxiety. Based on the answer (almost “never, sometimes, most of the time, almost” always), a score of one to four is assigned to the phrase with the highest score of four and the lowest score of one.15,16 The results of Spielberger questionnaire reliability showed a Cronbach’s alpha 0.76 for state and 0.85 for latent anxiety.
The Rosenberg self-esteem scale17 reliability test showed a 0.82 Cronbach’s alpha. This study used content validity to assess demographic characteristics. Experts reviewed and judged questions, including faculty members, psychiatrists, and psychologists. Mothers completed questionnaires in their health records and again after delivery. The results were incorporated into the study’s objectives and applied to the research.
Data analysis
The Kolmogorov-Smirnov test was used to determine if the data followed a normal distribution. Independent t-tests, chi-square tests, and Fisher’s exact tests were used to compare the socio-demographic characteristics of the intervention and control groups, and state and trait anxiety scores before the intervention. ANCOVA tests were used to compare anxiety scores while accounting for pre-intervention scores. A P value less than 0.05 was considered statistically significant, using SPSS-21 software.
Results
The study was started at April 2012 and ended in October 2012. 324 of the 424 pregnant women who attended health centers in the third trimester were not included in the study due to unwillingness, ineligibility, or history of severe depression. Finally, 100 women were included in this study. Figure 1 illustrates the process of the study. Two women from the control group (due to similar concerns faced by the control group) and two from the intervention group (due to emigration and preterm labor, respectively) were eliminated during the implementation phase. In the end, 48 women were left in the control group and the intervention group (see Figure 1). Regarding social and personal factors, there were no statistically significant differences between the intervention and control groups (P > 0.05). The mean age of participants in the intervention group was 24.34 (4.34) years, whereas those in the control group were 24.14 (3.86) years old. Obstetrics characteristics, such as the birth mode, newborn hospitalization, and gestational age at delivery time to weeks (based on early ultrasound) were similar in both groups (P > 0.05). The time of initial breastfeeding was shorter in peer support groups (P = 0.037).
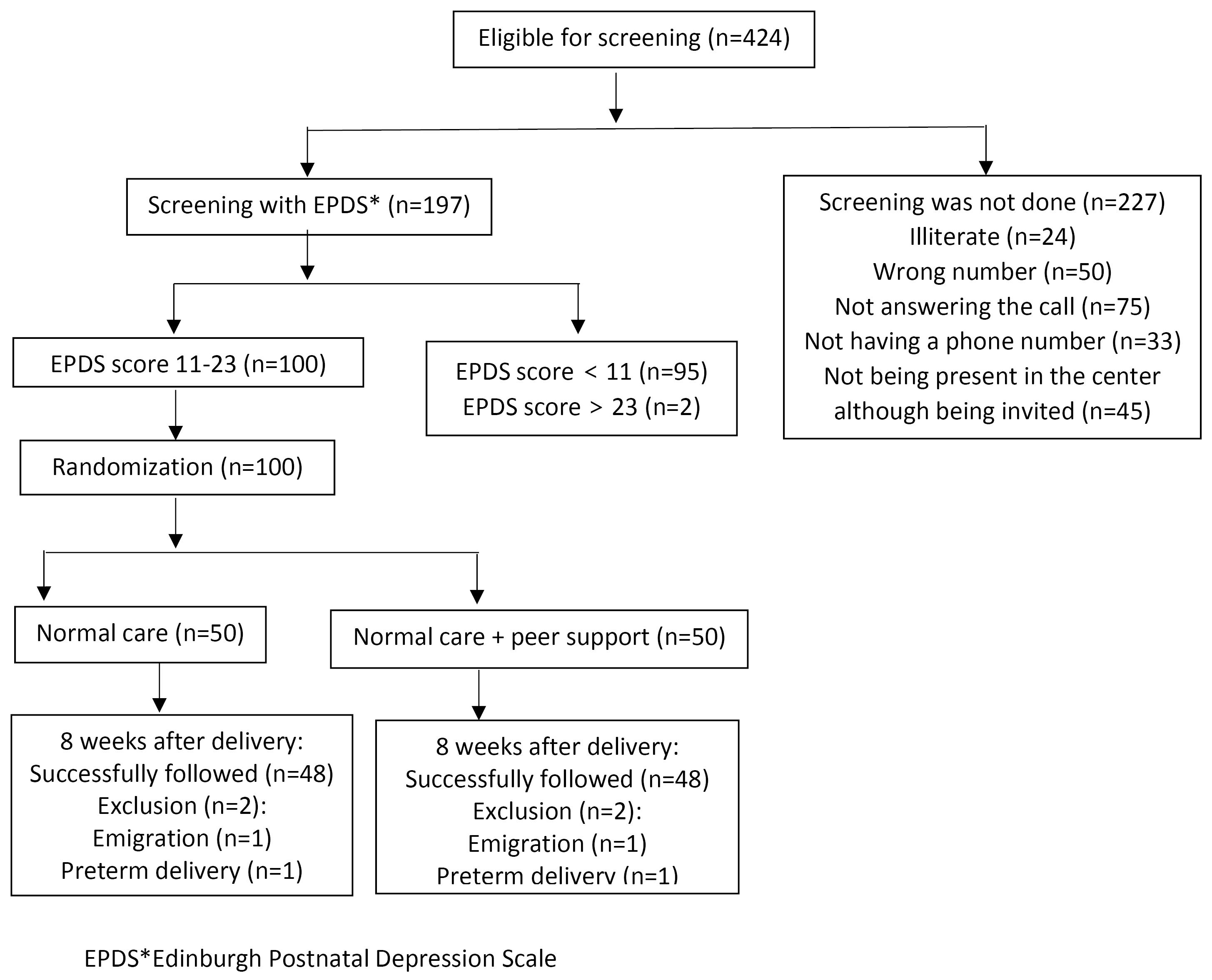
Figure 1.
Flow diagram of study participants
.
Flow diagram of study participants
Furthermore, 97.9% of mothers in the intervention group continued to breastfeed their infant two months after delivery using breast milk, compared to just 81.2% of mothers in the control group. This difference in breastfeeding rates was statistically significant (P = 0.027; Table 1). According to the data, 81.2% of the moms in the intervention group expressed pleasure, while 18.8% expressed no opinion. In the intervention group, the mean (SD) state anxiety score decreased significantly following intervention (P < 0.001); however, this reduction was not significant in the control group (P = 0.32). In terms of state anxiety, after adjusting for the pre-intervention level, there was a significant reduction in the peer support compared to the control group (P = 0.023) (see Table 2). When the pre-intervention trait anxiety score was taken into account, there was a statistically significant difference (P = 0.162) in trait anxiety across the groups (see Table 3). Although the self-esteem scores in both groups increased on average (SD), there was no statistically significant difference between the groups under study (P > 0.05; Table 4). After adjusting for the pre-intervention self-esteem level, the ANCOVA analysis revealed no significant difference (P = 0.87) between the groups (see Table 5).
Table 1.
Sociodemographic and obstetric characteristics of the participants in the control and intervention groups
|
Characteristic
|
Intervention (n=50) No. (%)
|
Control (n=50) No. (%)
|
P
value
|
| Agea |
24.34 (4.34) |
24.14 (3.86) |
0.80b |
| Maternal education |
|
|
0.88c |
| Primary |
10 (20) |
7 (14) |
|
| Secondary |
16 (32) |
18 (36) |
|
| Diploma |
21 (42) |
22 (44) |
|
| University |
3 (6) |
3 (6) |
|
| Paternal education |
|
|
0.04c |
| Primary |
11 (22) |
11 (22) |
|
| Secondary |
23 (46) |
13 (26) |
|
| Diploma |
16 (32) |
21 (42) |
|
| University |
0 (0) |
5 (10) |
|
| Maternal job |
|
|
0.88c |
| Housewife |
49 (98) |
48 (96) |
|
| Working at home |
1 (2) |
1 (2) |
|
| Working Outside |
0 (0) |
1 (2) |
|
| Preparing to take care of the child |
0.42c |
| completely |
14 (28) |
20 (40) |
|
| Somewhat |
31 (62) |
25 (50) |
|
| At least |
5 (10) |
5 (10) |
|
| Having spouse support |
0.24c |
| Yes |
45 (90) |
48 (96) |
|
| No |
5 (10) |
2 (4) |
|
Gestational age at
delivery time to
weeks (based on
early ultrasound)a |
39.3 (1.2) |
38.9 (1.2) |
0.06b |
| Delivery method |
|
|
0.30c |
| NVD |
29 (60) |
24 (50) |
|
| C/S |
19 (40) |
24 (50) |
|
| Neonate gender |
|
|
0.68c |
| Male |
24 (50) |
22 (46) |
|
| Female |
24 (50) |
26 (54) |
|
| Infant hospitalization |
0.27c |
| Yes |
6 (12.5) |
10 (21) |
|
| No |
42 (87.5) |
38 (79) |
|
| Time of first breastfeeding (h)a |
1.34 (0.49) |
1.57 (0.56) |
0.037b |
| Continuation of breastfeeding at 2 months |
0.027c |
| Breast milk |
47 (97.9) |
39 (81.2) |
|
| Breast and powdered milk |
1 (2.1) |
7 (14.6) |
|
| powdered milk |
0 (0) |
2 (4.2) |
|
aData were reported based on Mean (SD); b Independent t-test; c Chi-square test.
Table 2.
Anxiety score before and after intervention in control and intervention groups
|
Variables
|
Groups
|
Intervention Mean (SD)
|
Control Mean (SD)
|
| State anxiety |
Before intervention (n = 50) |
46.62 (7.8) |
44.39 (9.6) |
| 8 weeks after delivery (n = 48) |
40.64 (9.2) |
43.16 (9.17) |
| Statistical indicators |
t = 4.60; df = 47; P < 0.001 |
t = 0.99; df = 47; P = 0.32 |
| Trait anxiety |
Before intervention (n = 50) |
46.87 (8.2) |
45.47 (8.94) |
| 8 weeks after delivery (n = 48) |
42.5 (8.65) |
43.87 (8.2) |
| Statistical indicators |
t = 3.52; df = 47; P = 0.001 |
t = 1.36; df = 47; P = 0.17 |
Table 3.
Covariance analysis of the impact of peer support on postpartum anxiety
|
Source of changes
|
Total square
|
df
|
Mean square
|
F
|
P
value
|
Partial eta squared
|
| Pre-test state anxiety |
2189.99 |
1 |
2189.99 |
35.41 |
< 0.001 |
|
| Peer support |
331.54 |
1 |
331.54 |
5.36 |
0.023
|
0.055 |
| Error |
5751.6 |
93 |
61.6 |
|
|
|
| Pre-test trait anxiety |
2525.9 |
1 |
2525.9 |
42.8 |
< 0.001 |
|
| Peer support |
117.1 |
1 |
117.1 |
1.98 |
0.162 |
0.021 |
| Error |
5487 |
93 |
59 |
|
|
|
Table 4.
Self-esteem score before and after intervention in control and intervention groups
|
Groups
|
Intervention Mean (SD)
|
Control Mean (SD)
|
| Before intervention (n = 50) |
18.1 (3.9) |
18.1 (3.0) |
| 8 weeks after delivery (n = 48) |
18.9 (3.3) |
19.0 (3.6) |
| Statistical indicators |
t = 1.82; df = 47; P = 0.07 |
t = 1.77; df = 47; P = 0.08 |
Table 5.
Covariance analysis of the impact of peer support on self- confidence
|
Source of changes
|
Total square
|
df
|
Mean square
|
F
|
P
value
|
Partial eta squared
|
| Pre-test state anxiety |
400.73 |
1 |
400.73 |
50.79 |
< 0.001 |
|
| Peer support |
0.20 |
1 |
0.20 |
0.026 |
0.87 |
0.00 |
| Error |
5751.6 |
93 |
61.6 |
|
|
|
Discussion
Our study reveals that the intervention group’s state and trait anxiety scores dramatically dropped, while the control group showed no improvements. Following the intervention, the mean state anxiety level of the intervention group was considerably lower than that of the control group, even after adjusting for the pre-intervention anxiety score. There was no discernible variation in the self-esteem levels of the groups before and after the intervention. Compared to the control group, the intervention group’s time of beginning breastfeeding was shorter. Additionally, the intervention group’s rate of breastfeeding persistence at two months following delivery was statistically substantially greater than that of the control group.
In terms of mothers’ satisfaction about intervention, results showed that 81.2% of mothers in the intervention group were satisfied, while 18.8% had no opinion.
La Greca and Lopez, in their study examining the relationship between anxiety and groups of friends and peers among adolescent girls and boys, found that girls have higher anxiety than boys. Also, having relationships with peers reduced anxiety. This study has shown the effective role of peer support on reducing anxiety in line with ours.18
Another study focused on 143 expectant mothers and how prenatal therapies affected their feelings of sadness and anxiety. The mothers who received weekly phone support and a guidebook saw their anxiety drop significantly—from 40.8% to 6.4%. In contrast, the control group showed only a slight decrease in anxiety levels.19 Bullock et al also investigated the effects of late pregnancy on pregnant women and the role of telephone support. At 34 weeks of gestation, the intervention group’s self-esteem had increased due to weekly phone conversations.20 In Mashhad, Tafazzoli and team researched breastfeeding duration, comparing peer support with education from healthcare providers. They found no major differences in how quickly mothers started breastfeeding after giving birth among the three groups studied.21
Horton and colleagues looked at the effects of peer-to-peer phone counseling for patients with lupus. Among 153 participants, most were women who felt depressed and anxious. About 60% reported a change in how they viewed their illness, showing that peer counseling can be a helpful and cost-effective way to manage health-related stress.22
The results of a study by Wenzel et al. on the symptoms of postpartum anxiety on 147 women in the eighth week postpartum showed that the rate of anxiety increased in the postpartum period compared to the general population. About 10-50% of women show signs of postpartum anxiety, which is often associated with depression. In general, the prevalence of postpartum anxiety is higher than postpartum depression.23
Another study highlighted that postpartum anxiety is common in women, affecting 10%-50% of new mothers. Among 422 women with healthy infants, 24.9% had moderate anxiety. Factors like being young, single, or having a history of depression increased the risk of anxiety. Overall, anxiety and depression were found in 34% of the women studied.24-26
Pond and Kemp found a strong link between low self-esteem and high anxiety in both adolescents and adults.27 A quasi-experimental study showed that training given to women before leaving the hospital improved their self-esteem and reduced postpartum depression.28
A study with 70 first-time mothers showed that prenatal parenting education significantly lowered anxiety levels six weeks and six months after childbirth compared to those who did not receive the education.29
Given that anxiety during gestation constitutes a risk factor for negative outcomes for both mothers and offspring, the initiation of timely interventions has the potential to mitigate these issues. Considering the unique cultural context of our nation, which differs markedly from that of other countries, and the scarcity of research examining the effects of peer support on health outcomes—particularly for pregnant and lactating women—this investigation demonstrated a promising influence of peer support on postpartum anxiety among primiparous mothers. Nevertheless, this study was not without limitations. Specifically, mothers lacking a dedicated telephone line and residing with family members and spouses reported challenges in responding to calls from their peer mothers. This limitation represents a factor beyond the control of the researcher. Future studies should focus on mothers who have premature babies. Another limitation was that the mothers didn’t meet their peer supporters in person. To address this, future studies should try different ways of providing peer support, like in-person meetings or online groups.
Conclusion
The intervention group’s state and trait anxiety scores showed a considerable decrease, whereas the control group showed no discernible improvements. Additionally, there were no discernible variations in state anxiety levels between the intervention and control groups before the intervention. Following the intervention, the intervention group’s mean state anxiety score was statistically lower than the control group. On the other hand, a statistically significant difference in trait anxiety was noted between the groups. There was no discernible variation in the self-esteem levels of the groups before and after the intervention. Peer support has been shown to be beneficial in lowering postpartum anxiety, therefore regular prenatal care for expectant mothers should incorporate it.
Competing Interests
The authors certify that there is no conflict of interest with any financial organization regarding
the material discussed in the manuscript.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
All of the procedures were approved by the local ethical committee of Tabriz University of Medical Sciences and Ethics code (N0.33911). All procedures have been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki). This study was extracted from a master’s thesis that was registered at the Iranian Registry of Clinical Trials website (identifier: IRCT201202266582N7).
Informed Consent
Consent form was obtained from all participants.
Acknowledgements
This study is a part of an MSc dissertation conducted in the Nursing and Midwifery Faculty of Tabriz University of medical sciences. The authors are grateful for financial support from the research vice-chancellor of Tabriz University of Medical Sciences.
References
- Nelson AM. Transition to motherhood. J Obstet Gynecol Neonatal Nurs 2003; 32(4):465-77. doi: 10.1177/0884217503255199 [Crossref] [ Google Scholar]
- Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord 2016; 191:62-77. doi: 10.1016/j.jad.2015.11.014 [Crossref] [ Google Scholar]
- Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Curr Opin Psychiatry 2012; 25(2):141-8. doi: 10.1097/YCO.0b013e3283503680 [Crossref] [ Google Scholar]
- Nath S, Ryan EG, Trevillion K, Bick D, Demilew J, Milgrom J. Prevalence and identification of anxiety disorders in pregnancy: the diagnostic accuracy of the two-item generalized anxiety disorder scale (GAD-2). BMJ Open 2018; 8(9):e023766. doi: 10.1136/bmjopen-2018-023766 [Crossref] [ Google Scholar]
- Hasanjanzadeh P, Faramarzi M. Relationship between maternal general and specific-pregnancy stress, anxiety, and depression symptoms and pregnancy outcome. J Clin Diagn Res 2017; 11(4):VC04-7. doi: 10.7860/jcdr/2017/24352.9616 [Crossref] [ Google Scholar]
- Krol KM, Grossmann T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2018; 61(8):977-85. doi: 10.1007/s00103-018-2769-0 [Crossref] [ Google Scholar]
- Bollen A. Supporting women in the transition to motherhood: a research overview. Perspective 2015; 26:16-20. [ Google Scholar]
- Kruske S, Schmied V, Sutton I, O’Hare J. Mothers’ experiences of facilitated peer support groups and individual child health nursing support: a comparative evaluation. J Perinat Educ 2004; 13(3):31-8. doi: 10.1624/105812404x1752 [Crossref] [ Google Scholar]
- John HB, Philip RM, Santhanam S, Padankatti SM, Sebastian T, Balan I. Activity based group therapy reduces maternal anxiety in the neonatal intensive care unit - a prospective cohort study. Early Hum Dev 2018; 123:17-21. doi: 10.1016/j.earlhumdev.2018.07.001 [Crossref] [ Google Scholar]
- Consonni EB, Calderon IM, Consonni M, De Conti MH, Prevedel T, Rudge MV. A multidisciplinary program of preparation for childbirth and motherhood: maternal anxiety and perinatal outcomes. Reprod Health 2010; 7:28. doi: 10.1186/1742-4755-7-28 [Crossref] [ Google Scholar]
- Henderson AD. Henderson ADPreparing feminist facilitatorsAssisting abused women in transitional or support-group settings. J Psychosoc Nurs Ment Health Serv 1998; 36(3):25-33. doi: 10.3928/0279-3695-19980301-12 [Crossref] [ Google Scholar]
- Terry ML, Leary MR. Self-compassion, self-regulation, and health. Self Identity 2011; 10(3):352-62. doi: 10.1080/15298868.2011.558404 [Crossref] [ Google Scholar]
- Kamalifard M, Yavarikia P, Babapour Kheiroddin J, Salehi Pourmehr H, Iraji Iranagh R. The effect of peers support on postpartum depression: a single-blind randomized clinical trial. J Caring Sci 2013; 2(3):237-44. doi: 10.5681/jcs.2013.029 [Crossref] [ Google Scholar]
- Shahhosseini Z, Abedian K, Azimi H. Role of Anxiety During Pregnancy in Preterm Delivery. Journal of Advances in Medical and Biomedical Research 2008;16(63):85-92.[Persian].
- Speilberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. State-Trait Anxiety Inventory for Adults. Redwood City: Mind Garden Inc; 1983.
- Spielberger CD. State‐trait anxiety inventory. In: The Corsini Encyclopedia of Psychology. John Wiley & Sons; 2010.
- Rosenberg M. Rosenberg self-esteem scale (RSE). Acceptance and Commitment Therapy Measures Package 1965; 61(52):18. [ Google Scholar]
- La Greca AM, Lopez N. Social anxiety among adolescents: linkages with peer relations and friendships. J Abnorm Child Psychol 1998; 26(2):83-94. doi: 10.1023/a:1022684520514 [Crossref] [ Google Scholar]
- Milgrom J, Schembri C, Ericksen J, Ross J, Gemmill AW. Towards parenthood: an antenatal intervention to reduce depression, anxiety and parenting difficulties. J Affect Disord 2011; 130(3):385-94. doi: 10.1016/j.jad.2010.10.045 [Crossref] [ Google Scholar]
- Bullock LF, Wells JE, Duff GB, Hornblow AR. Telephone support for pregnant women: outcome in late pregnancy. N Z Med J 1995; 108(1012):476-8. [ Google Scholar]
- Tafazzoli M, moudi A, Boskabadi H, Ebrahim zadeh S. Comparing the Effect of Peer Support and the Education of Health Care Providers on Breastfeeding Initiation Time among Primiparous Women in Mashhad. The Iranian Journal of Obstetrics, Gynecology and Infertility 2012;15(4):19-28. [Persian].
- Horton R, Peterson MG, Powell S, Engelhard E, Paget SA. Users evaluate LupusLine, a telephone peer counseling service. Arthritis Care Res 1997; 10(4):257-63. doi: 10.1002/art.1790100407 [Crossref] [ Google Scholar]
- Wenzel A, Haugen EN, Jackson LC, Brendle JR. Anxiety symptoms and disorders at eight weeks postpartum. J Anxiety Disord 2005; 19(3):295-311. doi: 10.1016/j.janxdis.2004.04.001 [Crossref] [ Google Scholar]
- Britton JR. Pre-discharge anxiety among mothers of well newborns: prevalence and correlates. Acta Paediatr 2005; 94(12):1771-6. doi: 10.1111/j.1651-2227.2005.tb01852.x [Crossref] [ Google Scholar]
- Mirza I, Jenkins R. Risk factors, prevalence, and treatment of anxiety and depressive disorders in Pakistan: systematic review. BMJ 2004; 328(7443):794. doi: 10.1136/bmj.328.7443.794 [Crossref] [ Google Scholar]
- Taylor J, Johnson M. The role of anxiety and other factors in predicting postnatal fatigue: from birth to 6 months. Midwifery 2013; 29(5):526-34. doi: 10.1016/j.midw.2012.04.011 [Crossref] [ Google Scholar]
- Pond EF, Kemp VH. A comparison between adolescent and adult women on prenatal anxiety and self-confidence. Matern Child Nurs J 1992; 20(1):11-20. [ Google Scholar]
- Ahn YM, Kim MR. The effects of a home-visiting discharge education on maternal self-esteem, maternal attachment, postpartum depression and family function in the mothers of NICU infants. Taehan Kanho Hakhoe Chi 2004; 34(8):1468-76. doi: 10.4040/jkan.2004.34.8.1468 [Crossref] [ Google Scholar]
- Midmer D, Wilson L, Cummings S. A randomized, controlled trial of the influence of prenatal parenting education on postpartum anxiety and marital adjustment. Fam Med 1995; 27(3):200-5. [ Google Scholar]