J Res Clin Med. 13:33407.
doi: 10.34172/jrcm.025.33407
Original Article
Evaluation of diagnostic and therapeutic interventions in infants with head trauma in the north-west of Iran
Zhila Khamnian Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing, 1 
Ali Jafarizadeh Methodology, Project administration, Writing – original draft, Writing – review & editing, 2
Seyedehnastaran Hosseini Resources, Writing – review & editing, 2
Hamidreza Morteza Bagi Investigation, Resources, Supervision, Writing – review & editing, 3
Farhad Mirzaei Investigation, Resources, Supervision, Writing – review & editing, 4
Mirsaeed Abdollahi Formal analysis, Methodology, Writing – original draft, Writing – review & editing, 2, *
Author information:
1Department of Community Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
2Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
3Department of Emergency Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
4Department of Neurosurgery, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
This study explores the diagnostic and therapeutic procedures and their associated outcomes in infants with head trauma treated at the pediatric emergency department (ED) in northwest, Iran.
Methods:
A cross-sectional analysis was performed on one hundred children under one year of age, presenting with head trauma at Imam Reza Hospital from 2016 to 2019. Data included demographic characteristics and clinical manifestations.
Results:
Out of all infants, 62% were male. Falling from heights emerged as the most common etiology, accounting for 70% of incidents. Surgical consultation was performed for 59% of patients, and 22% required endotracheal intubation. Urinary and gastric catheterization were performed in 26% and 15% of cases, respectively. Arterial blood gas (ABG) tests were measured in 18% of patients. Of all patients, 37% were treated as outpatients and 13% were admitted to ICU. Study findings showed a significant association between mortality and gender, ABG tests, X-rays, the utility of NG tube and urinary catheter use, intubation, and fluid therapy (P<0.05). Noteworthy, there was no significant correlation between the cause of injury and patient mortality (P>0.05).
Conclusion:
Male infants exhibited a higher prevalence of head trauma. The mortality rate was also higher among male infants. The main cause of injury was falls from height. The majority of skull fractures were associated with epidural and subdural hematomas and intraventricular hemorrhage. A large number of patients were discharged on the same day. Mortality rates were higher among patients needing invasive treatment compared to those discharged after observation.
Keywords: Head trauma, Pediatric emergency department, Traumatic brain injury
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This study was not funded by any particular organization, company, etc.
Introduction
Childhood trauma is a predominant cause of mortality and morbidity, surpassing rates associated with congenital anomalies and pediatric oncological conditions. This trend is particularly pronounced in the demographic of children under the age of five.1,2 The main cause of trauma-related deaths in children is head trauma, underscoring its critical impact on child health. Head trauma in pediatric populations encompasses a spectrum of injuries to the scalp, skull, or brain, varying from minor contusions to severe forms of brain injury, such as traumatic brain injury (TBI), which is characterized by brain damage.3 Head trauma occurs commonly in infants and young children, with approximate annual rates of 1620 emergency department (ED) visits, 45 hospitalizations, and 4 deaths per 100 000 population in the United States.4 The higher rate of head trauma prevalence, particularly in younger children, imposes a significant economic burden on healthcare systems.4-7 The annual total costs associated with pediatric TBIs in the United States is approximately $667 million, with mean costs per TBI case being around $1532.3,7
The three leading causes of head trauma in children are falls from height, and car/bicycle accidents.8 Previous studies have also highlighted several clinical manifestations commonly associated with head trauma in infants, including altered mental status, loss of consciousness, caregiver-reported abnormal behavior, scalp hematoma, and vomiting. Furthermore, the occurrence of post-traumatic seizures has been linked to an increased likelihood of TBI. Additionally, skull fractures are noted in approximately 10% of cases involving infants with minor head trauma, which are mostly linear.9-11
Regarding the risk of developmental delays and behavioral problems in children following head trauma, multidisciplinary and early evaluation of diagnostic and therapeutic interventions is necessary. Neuroimaging, including ultrasound, computed tomography (CT) scan, and magnetic resonance imaging (MRI), plays a crucial role in the diagnosis of head trauma.12 Barlow et al evaluated the neurological and cognitive sequelae of late trauma in infants and found that the prognosis of head trauma at this age is poor and correlates with the severity of trauma. They suggested long-term follow-up of these infants in terms of learning and behavioral problems. Otherwise, the complications can be emerged in adolescents and youth.13
Considering the importance of both brain development in infancy and diagnostic examination in the management of trauma, this cross-sectional study was designed in the west-north of Iran to determine tailored procedures for the management of head trauma to prevent long-term complications and determine the prognosis of patients.
Materials and Methods
Study design and data collection
In the current cross-sectional study the medical records of all children under the age of one year who were referred to the child ED between April 2016 and April 2019 in northwest Iran were evaluated in accordance with the Helsinki Declaration and confirmation of the ethical committee of Tabriz University of medical science. Incomplete records that did not have a document of diagnostic procedures, such as tests or scans, were excluded. A checklist, used to collect data, has two sections: demographic (age, gender, etc.) and disease data (type of treatment, diagnosis, imaging findings, tests, treatments, including fluid therapy, etc).
Outcomes and variables
The study’s outcomes included evaluating the mortality rate, mechanism of trauma, and frequency of surgery consultations, ABG tests, X-rays, nasogastric (NG) tubes, foley catheter insertion, endotracheal intubation, and IV fluid prescriptions.
The categorical variables of the study were gender, clinical tests, intervention, etc., and quantitative variables such as age and admission days.
Statistical analysis
All data were analyzed using IBM SPSS version 26, and the Kolmogorov-Smirnov test was used to evaluate the normality of the collected data. According to the distribution of quantitative data, they were reported with mean, standard deviation, maximum, and minimum. We also reported nominal and ordinal data with frequencies and percentages. The chi-square or Fisher’s exact test was used to analyze the association between two variables.
Results
In this study, the medical records of one hundred children (< 1 year old) with head injuries referred to the ED of Imam Reza hospital, a trauma center in northwestern Iran, were assessed. The mean age was 152.85 ± 92.54 (min 3, max 330 days). 62% of the patients were males. The most common cause (70 %) of head trauma was falling from a height, while 30% resulted from hitting the head with a hard object like glass. Additionally, 33% of patients were reported without skull fractures. The frequency of fractures was reported as follows:
Skull fractures and epidural hematomas were 4, skull fractures with intracerebral and ventricular hemorrhage were 24, diffuse axonal injury (DAI) with cranial fractures were 10, mild subdural hemorrhage was 13, and Ping-Pong fractures were 16 patients (Figure 1).
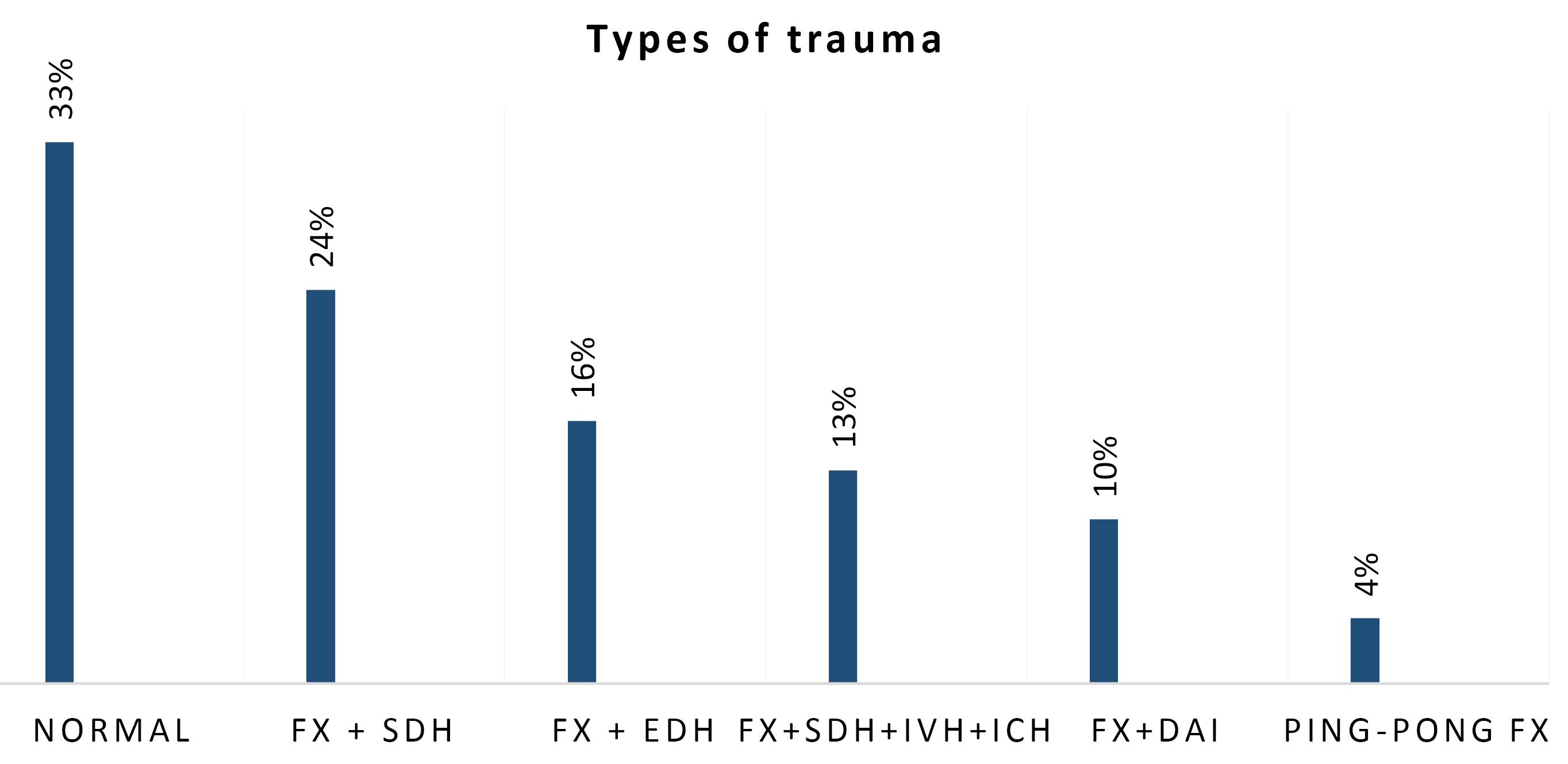
Figure 1.
Percentages of trauma and injuries. Abbreviations: Fx: fracture, EDH: epidural hematoma, SDH: subdural hematoma, IVH: intraventricular hemorrhage, ICH: intracerebral hemorrhage, DAI: diffused axonal injury
.
Percentages of trauma and injuries. Abbreviations: Fx: fracture, EDH: epidural hematoma, SDH: subdural hematoma, IVH: intraventricular hemorrhage, ICH: intracerebral hemorrhage, DAI: diffused axonal injury
The reports of ultrasound imaging, pulse oximetry, and ECG of all infants were normal at admission. Of note, no measurement of intracranial pressure was performed for any infant. The procedures performed for infants in the ED were listed in Table 1.
Table 1.
Procedures taken for infants in the emergency department
|
|
|
Frequency (percent)a
|
| Type of serum therapy |
No serum therapy |
36 |
| Dextrose saline |
20 |
| Normal saline |
36 |
| 1/3 2/3 b |
8 |
| Surgery consultation |
Yes |
59 |
| No |
41 |
| Intubation |
No |
78 |
| Yes |
22 |
| Urinary catheter insertion |
No |
74 |
| Yes |
26 |
| Insertion of gastric catheter |
No |
85 |
| Yes |
15 |
| Arterial blood gas |
No |
82 |
| Yes |
18 |
| Radiography |
Chest x-ray, Pelvic x-ray |
94 |
| Abnormal CT |
6 |
a According to the number of 100 infants in this study, the frequency and percentage are equal.
b composition: 3.3% dextrose and 0.3% sodium chloride solution
In this study, we observed that 67% of patients were admitted for treatment, whereas 33% received outpatient care and were subsequently discharged. The average duration of hospital admission was 3.3 days (SD = 2.49), with the mean stay in the ICU extending to 4 days (SD = 0.72). Notably, 13% of the patients required ICU admission. Among the total of 100 patients, 8 fatalities were recorded, all of whom were male and 4 patients were admitted to the ICU. Analysis of the gender distribution among the 33 discharged patients revealed that 63.6% were male (Figure 2), indicating a statistically significant association between patient mortality and gender (P = 0.023).
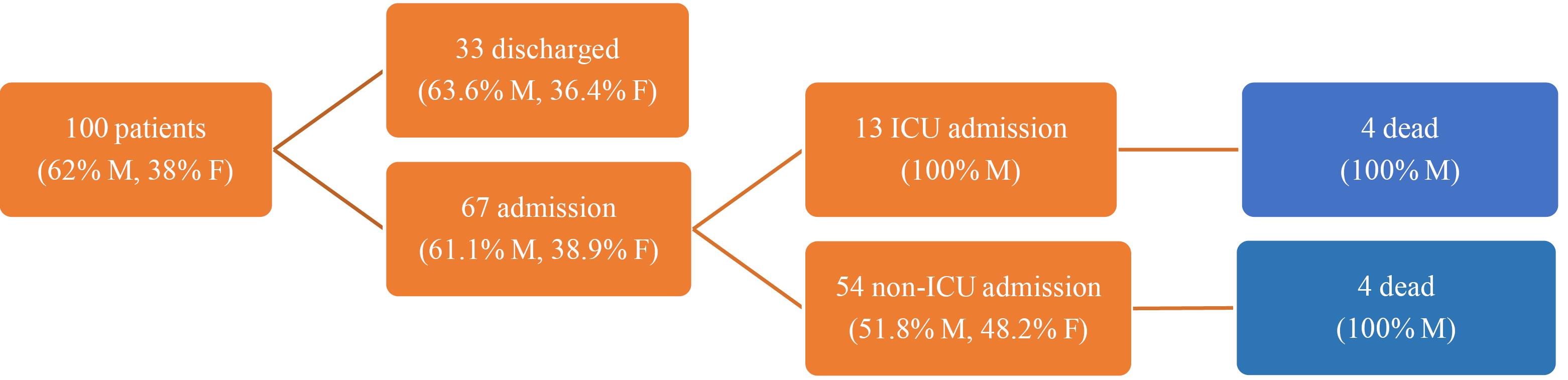
Figure 2.
General management
.
General management
Regarding the cause of injury, 50% of the deceased patients sustained injuries due to trauma with glass, while 50% were attributed to falls from height. Among the discharged patients, 71.74% incurred injuries due to falls and 28.26% from trauma with glass, indicating no significant relationship between the cause of injury and patient mortality (P = 0.23).
Fifty-nine patients underwent surgery consultation and 6.78% of these patients died, while 9.76% of the other group who did not undergo surgery consultation died. However, there was no statistically significant relationship between the mortality rate and surgery consultation (P = 0.71).
A noteworthy finding was the significant correlation between specific medical interventions and patient mortality. Patients requiring an arterial blood gas (ABG) test showed a significantly higher mortality rate, compared to those not needing the test (P = 0.033). The requirement for an NG tube was linked with a 40% mortality rate, compared to 2.35% in patients who did not need an NG tube (P < 0.001). Furthermore, 30.77% of patients with Foley catheters died (P < 0.001). The need for endotracheal intubation correlated with a 36.36% mortality rate against no deaths in patients not requiring intubation (P < 0.001) (Table 2).
Table 2.
Relationship between death and variables
|
Relationship between variables
|
P
value
|
| Gender |
0.023a |
| Mechanism of trauma |
0.23b |
| Surgery consultation |
0.71b |
| Arterial blood gas test |
0.033a |
| X-ray (Chest x-ray, pelvic x-ray) |
< 0.001a |
| Nasogastric tube |
< 0.001a |
| Foley catheter |
< 0.001a |
| Endotracheal tube |
< 0.001b |
| Intravenous fluid |
0.027b |
aFisher’s tests, bChi-square
Ultimately, the study examined the impact of fluid therapy on patient outcomes. According to the obtained results, the mortality rate in fluid therapy with Dextrose Water 5%, normal saline, and 1/3-2/3 IV fluids, was 20%, 11.11%, and 0%, respectively. There was no report of mortality in the patients who did not require fluid therapy. These findings suggest a significant relationship between the necessity of fluid therapy and patient mortality (P = 0.027).
Discussion
Previous studies have shown that the most common cause of death after trauma among children aged less than one year is head trauma.14,15 In the study by Arhami Dolatabadi et al in Tehran, among 547 children, 69.3% were male, and the most common cause of trauma and the injury site was car accidents (52.3%), and head and neck (39.7%), respectively.16 Also, the most common reason for head trauma was falling from heights. The authors noted that 537 patients were discharged with good general condition, 10 patients with trauma died, and the most common mortality was thoracic and abdominal trauma (14.3%); however, there was no statistically significant relationship between death and the mechanism of trauma and time of the accident. It has been reported that the most common type of trauma was in the male group under 14 years with a car accident from 7 pm to 12 am in the summer.16 Masoumi et al also reported that the mean age of head trauma was 18 months, 63 patients were male, and the most common cause was falling from heights,17 which is similar to our findings. Nnadi et al, in the evaluation of causes of head trauma in children, found that the most common type of trauma in newborn babies was falling, while pedestrian accidents were found in older children.18
Similar to our study, all of the dead patients were male, and 58.7% of the patients who were discharged were also males. There was a statistically significant relationship between the mortality rate and gender. Masoumi et al reported that the incidence of head trauma among males was more common, however, there was no statistically significant relationship between the abnormal CT scan findings and gender. Similar to the study conducted in Imam Hossein hospital, Tehran, no relationship between abnormal CT scan findings and the mechanism of trauma was found.17 Recurrent vomiting and decreased level of consciousness in patients with abnormal CT scans were higher than in the normal group, but there was no statistically significant difference between the groups. Therefore, they showed that vomiting and a decrease in the level of consciousness could not be considered for performing the CT scan. In line with our findings, they reported that most patients were discharged, and 18% of trauma ended in death.17
CT scan is a standard examination for intracranial injuries in children with head trauma19 and in the past decade, it has been increasingly used in children with head trauma.20 In the United States, 270 000 CT scans were performed in 1992.21 The data from pediatric EDs indicate that the rate of CT scan use for minor head injuries in children remained consistent at 32% between 2007 and 2015, despite educational efforts to decrease unnecessary use.22 However, more recent studies suggest a decline in CT scan utilization following the implementation of clinical guidelines. For instance, at the Children’s Hospital of Philadelphia, the rate of CT scan use for mild TBI decreased from 8.3% in 2012 to 4.9% in 2016 after adopting specific clinical pathways.23 In the United States and Canada, CT scan is performed in 15%-70% of children with head trauma who are admitted to the ED, while 70%-98% of these CT scans are normal and without any brain injury.24,25 In our study, X-ray was commonly used for outpatient infants.
In this era, Gruskin and Schutzman examined the prognostic factors of head trauma and showed that infants under one year had the highest incidence of skull fractures and intracranial injuries, and infants with a skull fracture, or intracranial injury showed more scalp abnormalities. Falling from a height ( < 0.9 m), maintaining alertness, having no history of neurological symptoms, and having a normal scalp examination were considered low-risk factors.26 In the current study, the prevalence of skull fractures with subdural hemorrhage was common. Barlow et al evaluated the neurological and cognitive sequelae of late trauma in infants and found that the prognosis of head trauma at this age is poor and correlates with the severity of trauma. Therefore, long-term follow-up of such infants has been suggested due to learning and behavioral problems. They have also pointed out that the early intervention in childhood can prevent clinical complications emerging in adolescents, and youth.13
A study by Meshkini et al also found that the most common symptom was vomiting. They also reported that blood glucose was significantly associated with a poor prognosis.27 Pineda et al found that changing the therapeutic protocols in the ICU can improve the outcomes and significantly decrease the mortality rate. The authors also found that the measurement of intracranial pressure with higher Glasgow coma scale (GCS) after resuscitation is accompanied by good outcomes.28 In our study, we did not measure the intracranial pressure of any infants. O’Lynnger et al showed that standardizing is associated with improved outcomes 4 times higher and decreased the mortality rate by 10 %.29 Bulger et al found that the admission time and mortality rate are lower in the centers with more invasive protocols. 30
Limitations and strengths
The strengths of this study include a comprehensive design, accurate data collection methods, and detailed analysis of results and variables. It is based on a cross-sectional analytical approach and provides an in-depth study of the documents of all children < 1 year of age referred to the ED over a three-year period. However, due to the limitations of this study in evaluating the child abuse possibility and parental education, we recommend further studies to address these unresolved issues.
Study Highlights
What is current knowledge?
What is new here?
-
Association between requirement for certain invasive medical interventions (e.g., arterial blood gas tests, nasogastric tube placement, urinary catheterization) and higher mortality rates.
Conclusion
Head trauma in male infants was more common than in females, with significant higher rate of neonatal mortality. The most common cause of head trauma was falling from a height. Most of the skull fractures were accompanied by epidural and subdural hematoma and intraventricular hemorrhage. The majority of the patients were discharged on the day of admission. The mortality rate was higher in patients who required invasive care and treatments, including ABG test, radiologic imaging, placing endotracheal or NG tube, and foley catheter. According to study findings, a systematic schedule needs to educate parents about the causes of trauma in infants, which is necessary to prevent and minimize the consequences of trauma in infants. Furthermore, early diagnostic modalities performed by child emergency specialists are necessary in preventive medicine toward infants’ health.
Competing Interests
The authors declare that there is no conflict of interest.
Ethical Approval
The medical ethics committee of the Tabriz University of Medical Science approved this study with the ethics code IR.TBZMED.REC.1398.728
Acknowledgements
We thank the neurosurgery and ED of the Imam Reza Hospital (Tabriz).
References
- Annegers JF. The epidemiology of head trauma in children. In: Shapiro I, ed. Pediatric Head Trauma. Mount Kisco, NY: Futura; 1983. p. 1-10.
- Dunn IF, Ellegala DB, Fox JF, Kim DH. Principles of cerebral oxygenation and blood flow in the neurological critical care unit. Neurocrit Care 2006; 4(1):77-82. doi: 10.1385/ncc:4:1:077 [Crossref] [ Google Scholar]
- Pinto PS, Meoded A, Poretti A, Tekes A, Huisman TAGM. The Unique Features of Traumatic Brain Injury in Children Review of the Characteristics of the Pediatric Skull and Brain, Mechanisms of Trauma, Patterns of Injury, Complications, and their Imaging Findings—Part 2. Journal of Neuroimaging 2012; 22(2):e18-e41. doi: 10.1111/j.1552-6569.2011.00690.x [Crossref] [ Google Scholar]
- Peterson AB, Xu L, Daugherty J, Breiding MJ. Surveillance Report of Traumatic Brain Injury-Related Emergency Department Visits, Hospitalizations, and Deaths, United States, 2014. National Center for Injury Prevention and Control; 2019.
- Coronado VG, Xu L, Basavaraju SV, McGuire LC, Wald MM, Faul MD. Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ 2011; 60(5):1-32. [ Google Scholar]
- Rahimi-Movaghar V, Saadat S, Rasouli MR, Ghahramani M, Eghbali A. The incidence of traumatic brain injury in Tehran, Iran: a population-based study. Am Surg 2011; 77(6):e112-4. [ Google Scholar]
- Shen J, Shi J, Cooper J, Chen C, Taylor HG, Xiang H. A population-based study of the incidence, medical care, and medical expenditures for pediatric traumatic brain injury. J Surg Res 2021; 268:87-96. doi: 10.1016/j.jss.2021.06.025 [Crossref] [ Google Scholar]
- Crankson SJ. Motor vehicle injuries in childhood: a hospital-based study in Saudi Arabia. Pediatr Surg Int 2006; 22(8):641-5. doi: 10.1007/s00383-006-1715-7 [Crossref] [ Google Scholar]
- Badawy MK, Dayan PS, Tunik MG, Nadel FM, Lillis KA, Miskin M. Prevalence of brain injuries and recurrence of seizures in children with posttraumatic seizures. Acad Emerg Med 2017; 24(5):595-605. doi: 10.1111/acem.13168 [Crossref] [ Google Scholar]
- Pandor A, Goodacre S, Harnan S, Holmes M, Pickering A, Fitzgerald P. Diagnostic management strategies for adults and children with minor head injury: a systematic review and an economic evaluation. Health Technol Assess 2011; 15(27):1-202. doi: 10.3310/hta15270 [Crossref] [ Google Scholar]
- Schutzman SA, Greenes DS. Pediatric minor head trauma. Ann Emerg Med 2001; 37(1):65-74. doi: 10.1067/mem.2001.109440 [Crossref] [ Google Scholar]
- Hedlund GL, Frasier LD. Neuroimaging of abusive head trauma. Forensic Sci Med Pathol 2009; 5(4):280-90. doi: 10.1007/s12024-009-9132-6 [Crossref] [ Google Scholar]
- Barlow KM, Thomson E, Johnson D, Minns RA. Late neurologic and cognitive sequelae of inflicted traumatic brain injury in infancy. Pediatrics 2005; 116(2):e174-85. doi: 10.1542/peds.2004-2739 [Crossref] [ Google Scholar]
- Trefan L, Houston R, Pearson G, Edwards R, Hyde P, Maconochie I. Epidemiology of children with head injury: a national overview. Arch Dis Child 2016; 101(6):527-32. doi: 10.1136/archdischild-2015-308424 [Crossref] [ Google Scholar]
- Søreide K, Krüger AJ, Ellingsen CL, Tjosevik KE. Pediatric trauma deaths are predominated by severe head injuries during spring and summer. Scand J Trauma Resusc Emerg Med 2009; 17:3. doi: 10.1186/1757-7241-17-3 [Crossref] [ Google Scholar]
- Arhami Dolatabadi A, Mohseninia N, Amiri M, Motamed H, Halimi Asl A. Pediatric trauma patients in Imam Hossein emergency department; an epidemiologic study. Iran J Emerg Med 2016; 3(1):4-8. doi: 10.22037/ijem.v3i1.10971 [Crossref] [ Google Scholar]
- Masoumi B, Heydari F, Hatamabadi H, Azizkhani R, Yoosefian Z, Zamani M. The relationship between risk factors of head trauma with CT scan findings in children with minor head trauma admitted to hospital. Open Access Maced J Med Sci 2017; 5(3):319-23. doi: 10.3889/oamjms.2017.071 [Crossref] [ Google Scholar]
- Nnadi MO, Bankole OB, Fente BG. Epidemiology and treatment outcome of head injury in children: a prospective study. J Pediatr Neurosci 2014; 9(3):237-41. doi: 10.4103/1817-1745.147577 [Crossref] [ Google Scholar]
- Maguire JL, Boutis K, Uleryk EM, Laupacis A, Parkin PC. Should a head-injured child receive a head CT scan? A systematic review of clinical prediction rules. Pediatrics 2009; 124(1):e145-54. doi: 10.1542/peds.2009-0075 [Crossref] [ Google Scholar]
- Osmond MH, Klassen TP, Wells GA, Correll R, Jarvis A, Joubert G. CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury. CMAJ 2010; 182(4):341-8. doi: 10.1503/cmaj.091421 [Crossref] [ Google Scholar]
- Mettler FA Jr, Wiest PW, Locken JA, Kelsey CA. CT scanning: patterns of use and dose. J Radiol Prot 2000; 20(4):353-9. doi: 10.1088/0952-4746/20/4/301 [Crossref] [ Google Scholar]
- Purcell L, Persson E, Houghton K. Curb unnecessary computed tomography scans for pediatric concussions. Can Fam Physician 2022; 68(9):667-9. doi: 10.46747/cfp.6809667 [Crossref] [ Google Scholar]
- Corwin DJ, Durbin DR, Hayes KL, Zonfrillo MR. Trends in emergent head computed tomography utilization for minor head trauma after implementation of a clinical pathway. Pediatr Emerg Care 2021; 37(9):437-41. doi: 10.1097/pec.0000000000001728 [Crossref] [ Google Scholar]
- Blackwell CD, Gorelick M, Holmes JF, Bandyopadhyay S, Kuppermann N. Pediatric head trauma: changes in use of computed tomography in emergency departments in the United States over time. Ann Emerg Med 2007; 49(3):320-4. doi: 10.1016/j.annemergmed.2006.09.025 [Crossref] [ Google Scholar]
- Servadei F, Vergoni G, Nasi MT, Staffa G, Donati R, Arista A. Management of low-risk head injuries in an entire area: results of an 18-month survey. Surg Neurol 1993; 39(4):269-75. doi: 10.1016/0090-3019(93)90003-j [Crossref] [ Google Scholar]
- Gruskin KD, Schutzman SA. Head trauma in children younger than 2 years: are there predictors for complications?. Arch Pediatr Adolesc Med 1999; 153(1):15-20. doi: 10.1001/archpedi.153.1.15 [Crossref] [ Google Scholar]
- Meshkini A, Salehpour F, Salimi Mehr N. Study of clinical signs and symptoms, laboratory tests in head trauma in children. Med J Tabriz Univ Med Sci Health Serv 2009; 31(2):95-9. [ Google Scholar]
- Pineda JA, Leonard JR, Mazotas IG, Noetzel M, Limbrick DD, Keller MS. Effect of implementation of a paediatric neurocritical care programme on outcomes after severe traumatic brain injury: a retrospective cohort study. Lancet Neurol 2013; 12(1):45-52. doi: 10.1016/s1474-4422(12)70269-7 [Crossref] [ Google Scholar]
- O’Lynnger TM, Shannon CN, Le TM, Greeno A, Chung D, Lamb FS. Standardizing ICU management of pediatric traumatic brain injury is associated with improved outcomes at discharge. J Neurosurg Pediatr 2016; 17(1):19-26. doi: 10.3171/2015.5.Peds1544 [Crossref] [ Google Scholar]
- Bulger EM, Nathens AB, Rivara FP, Moore M, MacKenzie EJ, Jurkovich GJ. Management of severe head injury: institutional variations in care and effect on outcome. Crit Care Med 2002; 30(8):1870-6. doi: 10.1097/00003246-200208000-00033 [Crossref] [ Google Scholar]