J Res Clin Med. 13:33344.
doi: 10.34172/jrcm.025.33344
Original Article
Identification of perivascular space dynamics with CT and MRI – Analysis with Hounsfield unit and point value measurements
Ziya Asan Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, * 
Aydan Koysuren Data curation, Formal analysis, Methodology, Resources, Supervision, Validation, Visualization, 2
Hatice Duygu Ciftci Sivri Formal analysis, Investigation, Methodology, Resources, Validation, 3
Author information:
1Department of Neurosurgery, Faculty of Medicine, Kirsehir Ahi Evran University, Kirsehir, Turkey
2Department of Neurology, Kirsehir Training and Research Hospital, Kirsehir, Turkey
3Department of Emergency Medicine, Kirsehir Training and Research Hospital, Kirsehir, Turkey
Abstract
Introduction:
This research aims to delineate the dynamic characteristics of perivascular spaces (PVS) using computed tomography (CT) and magnetic resonance imaging (MRI) examinations and to offer insights for differential diagnosis. Hounsfield Unit (HU) and point value measurements can aid in distinguishing PVS from other diagnosis.
Methods:
CT and MRI scans of patients diagnosed with PVS were retrieved from the radiology database. HU measurements were conducted on CT scans, while point value measurements were performed on T2-weighted MRI scans. Measurements of cerebrospinal fluid (CSF) HU and point values were also compared.
Results:
Evaluation of CT and MRI images from 117 cases revealed variability in HU and point value measurements of PVS across different imaging sessions, whereas no significant variability was noted in CSF. This underscores the homogeneous nature of CSF contrasted with the heterogeneous nature of PVS.
Conclusion:
PVS display a heterogeneous structure and possess distinct internal dynamics, differing from CSF. Despite their dynamic nature, PVS maintain consistent sizes and generally do not exert mass effects despite their cystic appearance.
Keywords: Computed tomography, Hounsfield unit, HU value, Magnetic resonance imaging, Perivascular space
Copyright and License Information
© 2025 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
There was no funding source for this study.
Introduction
Perivascular spaces (PVS), also known as Virchow-Robin spaces, are pial-lined structures that surround arteries and arterioles as they penetrate the cerebral parenchyma. They are typically observed in regions near the anterior commissure, the midbrain vertex, and the basal ganglia.1-3 While often microscopic in size intracranially, PVS can be visualized on radiological examinations when enlarged. While primarily asymptomatic, they may occasionally become symptomatic as they enlarge, potentially resulting in primary or secondary effects depending on their location.4-7 Diagnosis is commonly made following magnetic resonance imaging (MRI) examinations. Despite appearing iso-intense with cerebrospinal fluid (CSF) on imaging, histological examinations reveal differences in their contents compared to CSF. PVS exhibit a characteristic appearance based on their localization and radiological features. Despite their cystic appearance, they can be radiologically distinguished from other cystic formations by their lack of contrast retention on contrast-enhanced imaging and the absence of changes in size and imaging characteristics on repeated radiological examinations. When a differential diagnosis is challenging, it is essential to exclude other cystic structures from consideration.2-9
With the advancement of imaging techniques, there has been an increase in the frequency of diagnosing PVS. PVS are typically smaller than 5 mm and may not be identified in imaging studies with non-thin slices.10 Larger PVS, termed giant PVS, have the potential to become symptomatic.4,5,7,11 Although the exact etiology of giant PVS remains unknown, they are reported to be more prevalent in patients with dementia, epilepsy, hypertension, and head trauma.12-15
The aim of this study was to characterize the dynamic features of PVS in cases diagnosed with PVS using computed tomography (CT) and MRI examinations, utilizing Hounsfield Unit (HU) and point value measurements.
Materials and Methods
Cases diagnosed with PVS based on CT and MRI reports were identified by reviewing the radiology database at the institution where the study was conducted. Keyword filtering was applied using terms such as “PVS,” “perivascular space,” and “Virchow Robin space.” Subsequently, outpatient records of identified cases were scrutinized to document symptoms and indications for radiological examination. The records of 117 patients diagnosed with PVS and monitored since 2013 were retrospectively examined. Demographic information of the cases was documented by creating a database in an Excel file. CT and MRI scans of the cases were retrieved from the radiology database. Measurements were conducted using the picture archiving and communication system (PACS), and the sizes of PVS were recorded. In cases with multiple PVS, the largest one was evaluated for the study.
In CT examinations, the “point value” option was selected on the PACS software for detecting the HU value. The lowest and highest point values were obtained for the PVS. Similarly, in MRI imaging, the same technique was used to obtain the lowest and highest point values.
HU values of PVS and CSF were documented in CT examinations. In instances where follow-up CT examinations were conducted, HU values of both CSF and PVS were recorded for intergroup comparisons. For CSF HU value measurements, the highest and lowest HU values within the lateral ventricles were recorded. Regarding HU value measurements, the highest and lowest HU values were documented, and mean values were calculated. The disparity between the highest and lowest HU values of each structure was defined as the “heterogeneity index.” The disparities between CSF and PVS HU values, as well as the heterogeneity indices of CSF and PVS, were compared to ascertain differences in homogeneity between CSF and PVS.
Point value measurements were performed on the same structures assessed in MRI examinations (Figure 1). To accomplish this, axial T2 sequence images were analyzed using the PACS system. The disparity between point values was documented as the heterogeneity index.
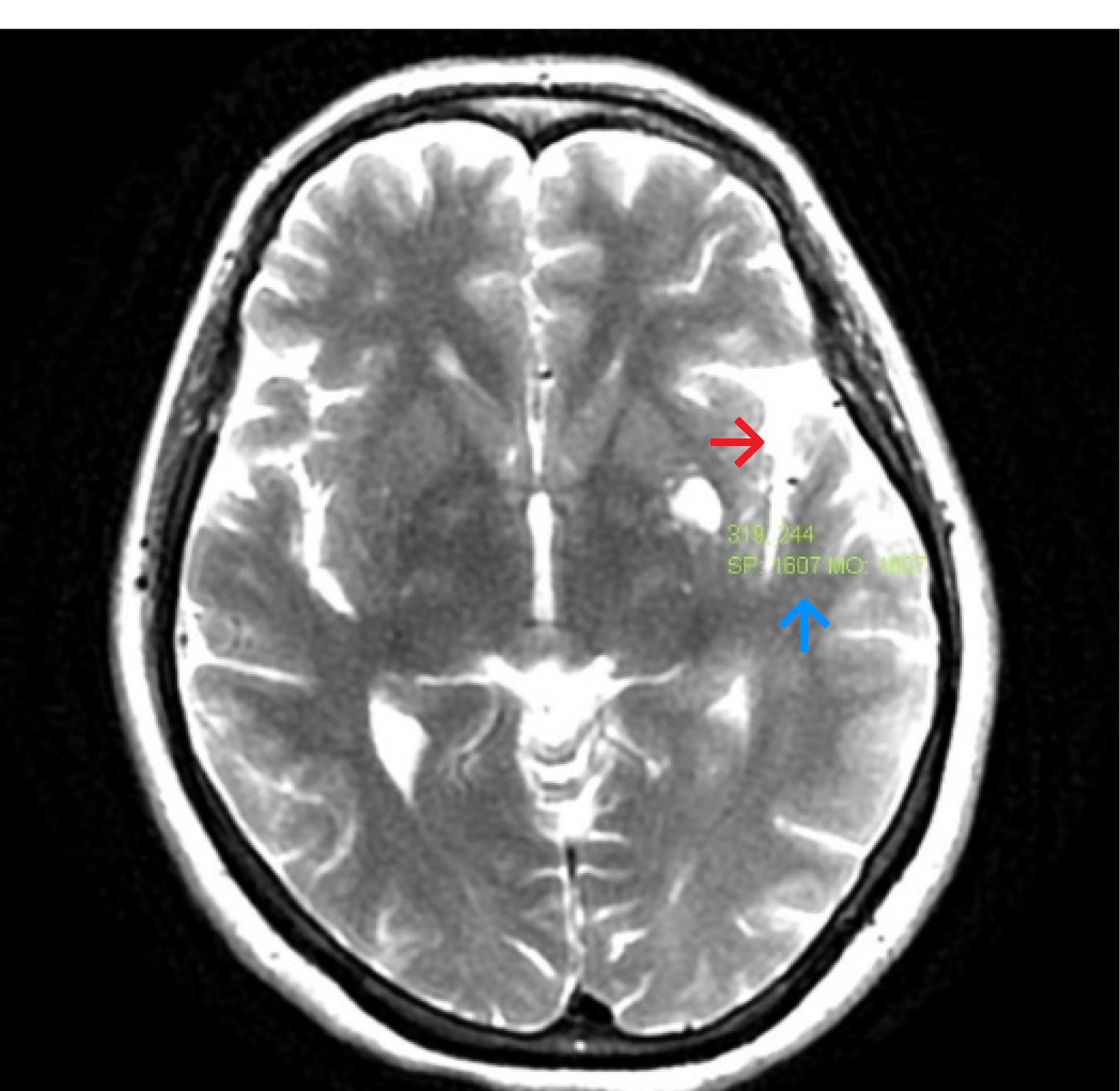
Figure 1.
Point value (red arrow) measurement of PVS (blue arrow) in T2-MRI imaging
.
Point value (red arrow) measurement of PVS (blue arrow) in T2-MRI imaging
Statistical analysis
The data of the cases were recorded in the database created in an Excel file and transferred to the SPSS 22 program for statistical analysis. Statistical calculations were performed, and to automate data entry for repeated computer operations, the WinAutomation Tool software was used. The Paired Samples t-test method was employed to compare the results of radiological examinations conducted at different times for the cases.
Results
A total of one hundred and seventeen cases meeting the study criteria were identified. The mean age of the cases was 45.17 ± 13.81 years, with 69 being male and 48 female. Diagnosis was incidentally made following cranial CT examinations in 67 cases after head trauma. It was found that 66 patients received medical treatment for hypertension. Diagnosis was made for 14 cases following radiological examinations due to dizziness. One case was diagnosed following investigations for ischemic cerebrovascular disease. A large PVS exhibiting cavitation at the level of the mesencephalon was observed in one case (Figure 2). Symptoms of anisocoria and right mild hemiparesis were also documented in this case.
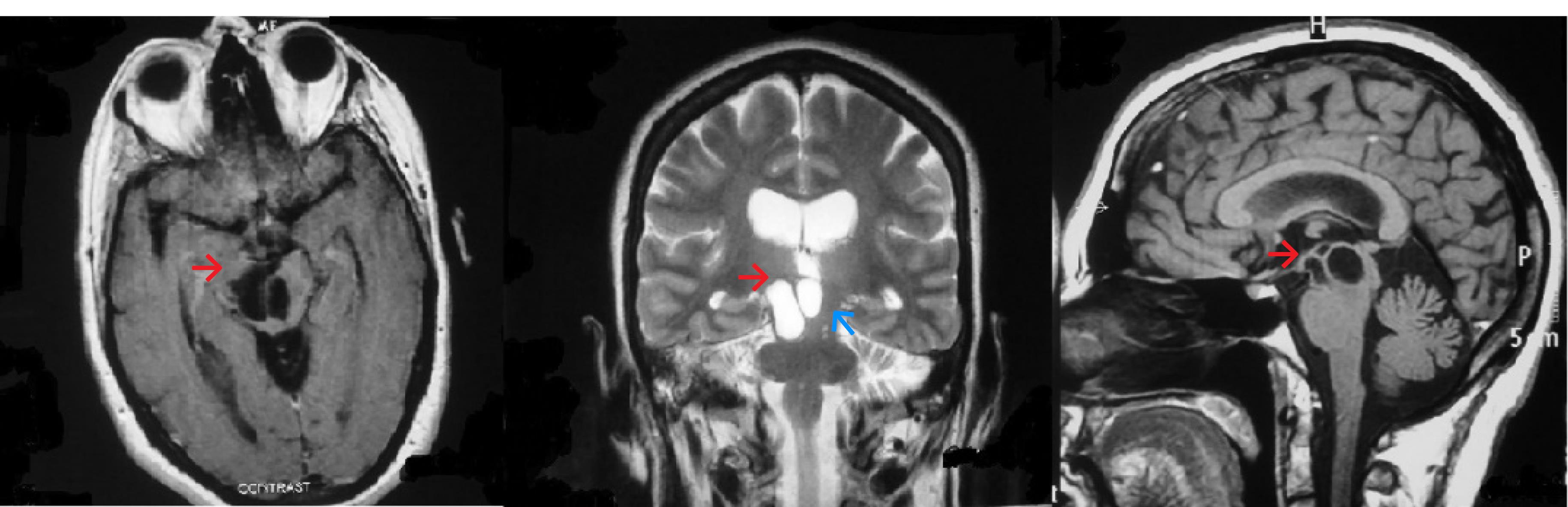
Figure 2.
Giant PVS with septation at the level of the mesencephalon (a,b,c: red arrow). PVS does not cause a significant mass effect (blue arrow)
.
Giant PVS with septation at the level of the mesencephalon (a,b,c: red arrow). PVS does not cause a significant mass effect (blue arrow)
Control CT scans were conducted for 47 cases, while control MRI examinations were performed for 70 cases. The interval between radiological examinations in cases evaluated by CT was calculated as 19.49 ± 7.13 months, whereas it was 12.39 ± 4.96 months in cases evaluated by MRI.
The mean HU value of CSF on initial CT examinations was calculated as 2.33 ± 1.04, while the mean HU value of PVS was 12.38 ± 1.11. The heterogeneity index of CSF was 15.89 ± 1.67, whereas that of PVS was 18.34 ± 2.11. PVS were found to be significantly more heterogeneous than CSF (P = 0.009). On follow-up CT examinations, the mean HU value of CSF was 2.16 ± 0.73, and that of PVS was 11.43 ± 0.37. Although no significant difference was observed in the heterogeneity index of CSF, it was determined that the heterogeneity of PVS significantly changed (P = 0.015). Specifically, the heterogeneity index increased in 27 cases and decreased in 20 cases.
On initial axial T2-weighted MRI examinations of cases evaluated by MRI, the mean score of CSF was 1342.42 ± 5.23, and that of PVS was 1330.31 ± 88.75. On follow-up MRI examinations, the mean score of CSF was 1331 ± 5.73, and that of PVS was 1358.32 ± 14.58. Significant changes in the heterogeneity of PVS were detected on MRI examinations (P = 0.008).
HU values of CT images and their differences are shown in Table 1, and point value differences of MRI are presented in Table 2.
Table 1.
Differences between CSF and PVS HU values according to CT examinations
|
|
First CT
|
Control CT
|
P
value
|
| Lateral ventricle Mean HU |
2.33 ± 1.04 |
2.16 ± 0.73 |
0.363 |
| PVS mean HU |
12.38 ± 1.11 |
11.43 ± 0.37 |
0.042 |
| Lateral ventricular heterogeneity index |
15.89 ± 1.67 |
15.81 ± 1.99 |
0.808 |
| PVS heterogeneity index |
18.34 ± 2.11 |
15.59 ± 0.83 |
0.015 |
CT: computed tomography; CSF: cerebrospinal fluid; PVS: perivascular space.
Table 2.
Differences between CSF and PVS HU values according to MRI examinations
|
|
First MRI
|
Control MRI
|
P
value
|
| CSF Mean PV |
1342.42 ± 5.23 |
1331 ± 5.73 |
0.150 |
| PVS mean PV |
1330.31 ± 88.75 |
1358.32 ± 14.58 |
0.023 |
| Lateral ventricular heterogeneity index |
609.36 ± 92.97 |
636.21 ± 102.39 |
0.095 |
| PVS heterogeneity index |
923.84 ± 133.23 |
977.87 ± .09 |
0.029 |
MRI: magnetic resonance imaging; CSF: cerebrospinal fluid; PVS: perivascular space; PV: point value.
Discussion
PVS are typically benign formations that are often incidentally detected. They exhibit typical imaging characteristics, and their precise localization aids in the process of differential diagnosis.16-18 PVS are recognized to exhibit the same intensity as CSF on MRI examinations. They are predominantly located in the subcortical regions of the basal ganglia and are often termed “sublenticular cysts.” Typically small in size, they are commonly asymptomatic. However, in some instances, the detection of large PVS formations can result in a compressive effect, leading to symptomatic manifestations.5,11 Cases of PVS causing obstructive hydrocephalus and homonymous quadrantanopia due to compression on the optic tract have been reported.5,6 Additionally, it has been reported that PVS detected in adult cases can lead to cognitive function deterioration.12,14 Differential diagnoses for PVS include lacunar infarction, cystic periventricular leukomalacia, multiple sclerosis, cryptococcosis, mucopolysaccharidoses, cystic neoplasms, neurocysticercosis, arachnoid cysts, and neuroepithelial cysts.16-18 Further radiological examinations are helpful in the differential diagnosis of PVS. There are no specific additional laboratory findings to support the diagnosis of PVS. Therefore, in cases where a differential diagnosis is required, it is essential to exclude other possible diagnoses through comprehensive evaluation.
Today, the widespread utilization of PACS in radiological assessments allows for the acquisition of qualitative data in tissue radiological examinations. HU value measurements in CT examinations serve as a quantitative assessment method, measuring the X-ray absorption of tissues. Given that different tissues possess distinct HU values, a differential diagnosis can be facilitated between radiologically similar tissues by utilizing data obtained from these values. HU value measurements represent pixel values of colors. Therefore, even if a tissue appears to be quantitatively homogeneous, equal HU values may not be obtained in every region of the tissue. The more homogeneous the tissue, the fewer anticipated differences in HU values. The term “heterogeneity index” was defined by the senior author to denote the difference in HU values between different tissue regions. A high value of this index indicates that the tissue exhibits significant heterogeneity.
Point value measurements on MRI examinations, similar to HU measurements in CT scans, can provide insights into color values. Similarly, it is acknowledged that greater tissue homogeneity is associated with a lower heterogeneity index.
CSF is expected to exhibit homogeneity under normal conditions due to its continuous circulation. Therefore, the disparity between HU values in CT examinations and point values in MRI examinations is anticipated to be minimal. Consequently, in homogeneous structures, the heterogeneity index should be lower. PVS appear hypodense on CT examinations and hyperintense on T2-weighted sequences in MRI examinations. While this characteristic can also be observed in CSF, quantitative measurements in CT and MRI enable a qualitative assessment and comparison of the hypodensity or hyperintensity of these tissues.
Upon evaluating CT and MRI examinations of PVS cases, significant differences were noted between both HU values in CT and point values in MRI examinations. Radiological measurements of these structures, which are quantitatively similar but qualitatively different, suggest that the contents of these structures are also distinct. The lack of significant changes in the HU and point values of CSF in radiological examinations conducted at different times indicates that there is no alteration in the homogeneity of CSF. However, significant qualitative differences were demonstrated in the radiological evaluations of PVS at different time points. This data serves as a qualitative indicator of changes occurring within the structure of PVS over time.
In quantitative radiological evaluations of PVS, it is observed that they do not generate a significant mass effect in the region where they are detected and do not exert compression on neighboring structures. This data suggests that PVS have a cavitary form and do not induce any dimensional alterations. However, compared to CSF, the heterogeneity index in PVS was significantly higher. This also suggests that PVS possess their own internal dynamics.
Although significant changes in the homogeneity of PVS were detected in radiological examinations, it is proposed that their internal dynamics are limited to the extent that they cannot induce a notable change in PVS dimensions. Until equal homogeneity is achieved between the two fluids, different forms of osmotic activity between adjacent fluid structures are expected to occur. The absence of size changes in PVS indicates that osmotic processes do not occur within PVS. This supports the notion that PVS exhibit internal dynamics independent of surrounding tissues but do not lead to significant mass activity.
Histological examinations also provide insight into the internal dynamics of PVS. However, given that PVS are almost always situated in critical areas, it should be noted that a diagnostic surgical approach to these structures would entail very high morbidity.
Study Highlights
What is current knowledge?
What’s new here?
Conclusion
The observation of HU and point values of PVS in radiological examinations conducted at different times suggests the presence of internal dynamics in these structures. However, the internal dynamics of PVS are restricted to the point where they cannot generate dimensional differences. Changes in heterogeneity serve as indicators of alterations in their internal dynamics.
Competing Interests
The authors declare no conflict of interest.
Ethical Approval
This study obtained ethical approval from the Clinical Research Ethics Committee of Ahi Evran University with decision number 20-18-05/48. As the study is retrospective in nature, patient consent was not obtained.
Acknowledgements
The authors would like to express their gratitude to Omer Asan and Nurhale Asan for their assistance in writing the article and collecting the data.
References
- Sadashiva N, Saini J. Dilated Virchow Robin spaces in brainstem. Br J Neurosurg 2023; 37(3):307-8. doi: 10.1080/02688697.2020.1817854 [Crossref] [ Google Scholar]
- Wang G. Perivascular space and neurological disorders. Neurosci Bull 2009; 25(1):33-7. doi: 10.1007/s12264-009-1103-0 [Crossref] [ Google Scholar]
- Saeki N, Sato M, Kubota M, Uchino Y, Murai H, Nagai Y. MR imaging of normal perivascular space expansion at midbrain. AJNR Am J Neuroradiol 2005; 26(3):566-71. [ Google Scholar]
- Thirumurthi T, Abdelrahman M, Kanodia AK, Elmaadawi I, Torgersen A, Rajendra J. Giant perivascular space: a rare cause of acute neurosurgical emergency. Br J Neurosurg 2023; 37(6):1699-703. doi: 10.1080/02688697.2020.1823942 [Crossref] [ Google Scholar]
- Ayele B, Zenebe G, Mengesha A, Teshale Y. Symptomatic giant Virchow-Robin spaces: a rare cause of spastic quadriparesis in 43-year-old Ethiopian patient: a case report. Ethiop J Health Sci 2020; 30(5):843-6. doi: 10.4314/ejhs.v30i5.24 [Crossref] [ Google Scholar]
- Woo PY, Cheung E, Zhuang JT, Wong HT, Chan KY. A giant tumefactive perivascular space: a rare cause of obstructive hydrocephalus and monoparesis. Asian J Neurosurg 2018; 13(4):1295-300. doi: 10.4103/ajns.AJNS_108_18 [Crossref] [ Google Scholar]
- Austein F, Langguth P, Lindner T. Extreme widening of asymmetric giant cystic Virchow-Robin spaces. Neuroradiology 2018; 60(1):3-5. doi: 10.1007/s00234-017-1951-7 [Crossref] [ Google Scholar]
- Saylisoy S, Simsek S, Adapinar B. Is there a connection between perivascular space and subarachnoid space?. J Comput Assist Tomogr 2014; 38(1):33-5. doi: 10.1097/RCT.0b013e3182a9a45a [Crossref] [ Google Scholar]
- Wang P, Olbricht WL. Fluid mechanics in the perivascular space. J Theor Biol 2011; 274(1):52-7. doi: 10.1016/j.jtbi.2011.01.014 [Crossref] [ Google Scholar]
- Sung J, Jang J, Choi HS, Jung SL, Ahn KJ, Kim BS. Linear sign in cystic brain lesions ≥ 5 mm: a suggestive feature of perivascular space. Eur Radiol 2017; 27(11):4747-55. doi: 10.1007/s00330-017-4878-9 [Crossref] [ Google Scholar]
- Yılmaz G, Akpınar S. Enlarged perivascular space mimicking mesencephalothalamic cystic tumor. Iran J Neurol 2014; 13(4):253-4. [ Google Scholar]
- Shin NY, Park YW, Yoo SW, Yoo JY, Choi Y, Jang J. Adverse effects of hypertension, supine hypertension, and perivascular space on cognition and motor function in PD. NPJ Parkinsons Dis 2021; 7(1):69. doi: 10.1038/s41531-021-00214-6 [Crossref] [ Google Scholar]
- Sepehrband F, Barisano G, Sheikh-Bahaei N, Choupan J, Cabeen RP, Lynch KM. Volumetric distribution of perivascular space in relation to mild cognitive impairment. Neurobiol Aging 2021; 99:28-43. doi: 10.1016/j.neurobiolaging.2020.12.010 [Crossref] [ Google Scholar]
- Huang P, Zhu Z, Zhang R, Wu X, Jiaerken Y, Wang S. Factors associated with the dilation of perivascular space in healthy elderly subjects. Front Aging Neurosci 2021; 13:624732. doi: 10.3389/fnagi.2021.624732 [Crossref] [ Google Scholar]
- Wang H, Nie ZY, Liu M, Li RR, Huang LH, Lu Z. Clinical characteristics of perivascular space and brain CT perfusion in stroke-free patients with intracranial and extracranial atherosclerosis of different extents. Ann Transl Med 2020; 8(5):215. doi: 10.21037/atm.2020.01.35 [Crossref] [ Google Scholar]
- Ramirez J, Holmes MF, Berezuk C, Kwan D, Tan B, Beaton D. MRI-visible perivascular space volumes, sleep duration and daytime dysfunction in adults with cerebrovascular disease. Sleep Med 2021; 83:83-8. doi: 10.1016/j.sleep.2021.03.043 [Crossref] [ Google Scholar]
- Barisano G, Law M, Custer RM, Toga AW, Sepehrband F. Perivascular space imaging at ultrahigh field MR imaging. Magn Reson Imaging Clin N Am 2021; 29(1):67-75. doi: 10.1016/j.mric.2020.09.005 [Crossref] [ Google Scholar]
- Ramirez J, Berezuk C, McNeely AA, Gao F, McLaurin J, Black SE. Imaging the perivascular space as a potential biomarker of neurovascular and neurodegenerative diseases. Cell Mol Neurobiol 2016; 36(2):289-99. doi: 10.1007/s10571-016-0343-6 [Crossref] [ Google Scholar]